
Top Essay Writers
Our top essay writers are handpicked for their degree qualification, talent and freelance know-how. Each one brings deep expertise in their chosen subjects and a solid track record in academic writing.
Simply fill out the order form with your paper’s instructions in a few easy steps. This quick process ensures you’ll be matched with an expert writer who
Can meet your papers' specific grading rubric needs. Find the best write my essay assistance for your assignments- Affordable, plagiarism-free, and on time!
Posted: July 14th, 2022
CHAPTER ONE
Little is known about the psychobiological processes of adults, at age 23, who
We get a lot of “Can you do MLA or APA?”—and yes, we can! Our writers ace every style—APA, MLA, Turabian, you name it. Tell us your preference, and we’ll format it flawlessly.
were born prematurely despite the fact that 1 out of every 9 infants is born too early
(Atzil, Hendler & Feldman, 2011; CDC, 2015; Mannisto, Vaarasmaki, Sipola –
Leppanen, Tikanmaki, Matinolli, Pesonen, Raikkonen, Jarvelin, Hovi, & Kajantie,
2015). Compared to infants born at term, premature infants, face additional obstacles
Totally! They’re a legit resource for sample papers to guide your work. Use them to learn structure, boost skills, and ace your grades—ethical and within the rules.
of immature body systems and more neonatal stress, and are at risk for developmental
delay, and possible parental overprotection patterns (Clarke, Cooper & Creswell,
2013; Grunau, 2013; Kopp & Rethelyi, 2003; Pinquart, 2014).
Starts at $10/page for undergrad, up to $21 for pro-level. Deadlines (3 hours to 14 days) and add-ons like VIP support adjust the cost. Discounts kick in at $500+—save more with big orders!
Developmentally, in the United States, 23 year olds are expected to achieve
independence and form intimate relationships, yet there is limited knowledge about
their emotional intelligence and related psychobiological processes while more is
known about their stress levels, coping strategies, and emotional disorders (Clarke, et
100%! We encrypt everything—your details stay secret. Papers are custom, original, and yours alone, so no one will ever know you used us.
al, 2013; Ingels, Glennie, Lauff, & Wirt, 2012; Pinquart, 2014; Simpson, 2009).
Intrapersonal, interpersonal, adaptability, stress management effectiveness, as well as
general emotional health are all involved in reaching adult developmental milestones
(Granger & Kivlighan, 2003; Simpson, 2009). These important young adults
Nope—all human, all the time. Our writers are pros with real degrees, crafting unique papers with expertise AI can’t replicate, checked for originality.
milestones require the ability to: communicate effectively with others, be sensitive to
others, maintain emotional self-control, use both knowledge and experiences to cope,
manage stress, work and assume responsibilities (Arnett, 2013; Di Fabio & Saklofse,
2014; Simpson, 2009).
Our writers are degree-holding pros who tackle any topic with skill. We ensure quality with top tools and offer revisions—perfect papers, even under pressure.
The abilities required to meet young adult developmental milestones are captured
in definitions of emotional intelligence (EI) and also incorporates the involvement of
the brain’s prefrontal cortex executive functioning which further evolves during this
time period (Kristensen, Parker, Taylor, Keefer, Kloosterman, & Summerfeldt, 2014;
Experts with degrees—many rocking Master’s or higher—who’ve crushed our rigorous tests in their fields and academic writing. They’re student-savvy pros, ready to nail your essay with precision, blending teamwork with you to match your vision perfectly. Whether it’s a tricky topic or a tight deadline, they’ve got the skills to make it shine.
Arnett, 2013; Davis & Humphrey, 2012; Armstrong, Galligan, & Critchley, 2011;
Lishner, Swim, Hong & Vitacco, 2011; Aldao, Nolen-Hoeksema & Schweizer, 2010;
Stuss, 2009; Tarasuik, Ciorciari & Stough, 2009; Ciarrochi, Deane & Anderson,
2000). The Hypothalamic – Pituitary -Adrenal (HPA) Axis biological response to
Guaranteed—100%! We write every piece from scratch—no AI, no copying—just fresh, well-researched work with proper citations, crafted by real experts. You can grab a plagiarism report to see it’s 95%+ original, giving you total peace of mind it’s one-of-a-kind and ready to impress.
stress and prefrontal cortex executive functioning abilities are theorized to be involved
with emotional intelligence (EI), functioning, stress, coping, and emotional health
(Frodl & Stuart, & Pretorius, 2007; Smith & Vale, 2006; Herman, Ostrander, Meuller
& Figueiredo, 2005).
Yep—APA, Chicago, Harvard, MLA, Turabian, you name it! Our writers customize every detail to fit your assignment’s needs, ensuring it meets academic standards down to the last footnote or bibliography entry. They’re pros at making your paper look sharp and compliant, no matter the style guide.
Young adults who were born prematurely carry the consequences of their early
birth. As infants, their immature physical systems were responding to ongoing
physical pain from neonatal medical procedures, a longer hospitalization and a
multitude of environmental stimuli with unstable and ineffective bodily system
For sure—you’re not locked in! Chat with your writer anytime through our handy system to update instructions, tweak the focus, or toss in new specifics, and they’ll adjust on the fly, even if they’re mid-draft. It’s all about keeping your paper exactly how you want it, hassle-free.
responses (Grunau, 2002). The foundations for brain growth and functioning and
what will become their usual stress response were being laid at this point in time and
will likely influence lifelong development including meeting young adult milestones.
However, there is a need for research examining the mechanisms of stress and its
It’s a breeze—submit your order online with a few clicks, then track progress with drafts as your writer brings it to life. Once it’s ready, download it from your account, review it, and release payment only when you’re totally satisfied—easy, affordable help whenever you need it. Plus, you can reach out to support 24/7 if you’ve got questions along the way!
relationship with adult emotional health outcome to assure the well being of young
adults and their attainment of developmental milestones (Mannisto, et al., 2015;
Simpson, 2009; Tarasuik, et al., 2009). There is minimal research into emotional
health and its association with biological processes functioning existing to help in
Need it fast? We can whip up a top-quality paper in 24 hours—fully researched and polished, no corners cut. Just pick your deadline when you order, and we’ll hustle to make it happen, even for those nail-biting, last-minute turnarounds you didn’t see coming.
identifying the precise timing and targets of health promoting interventions.
Theoretical Framework
The Developmental Origins of Health and Disease (DOHaD) theory of HPA
dysregulation postulates that the stress of prematurity and during early life critical
brain growth periods (i.e. formation completes during young adulthood) effects the
Absolutely—bring it on! Our writers, many with advanced degrees like Master’s or PhDs, thrive on challenges and dive deep into any subject, from obscure history to cutting-edge science. They’ll craft a standout paper with thorough research and clear writing, tailored to wow your professor.
HPA Axis structure and functioning (Eiland & McEwen, 2012; Sullivan, Hawes,
Winchester & Miller, 2008; Barker, 2007; Miller, Chen & Zhou, 2007; De Boo &
Harding, 2006; Pujol, Vendrell, Junque, Marti-Vilalta, & Capdevila, 1993). Stress
responses from the HPA axis are adaptive (allostasis) and if occur frequently,
particularly with prematurely born infants and their underdeveloped systems, will
We follow your rubric to a T—structure, evidence, tone. Editors refine it, ensuring it’s polished and ready to impress your prof.
result in injury or ‘”wear and tear” (allostatic load) on the body (McEwen, 2003 &
2006; McEwen & Seeman, 2006). If the stress is ongoing or chronic than the “wear
and tear” on the body will result in illness (McEwen, 2003 & 2006 McEwen &
Seeman, 2006). Cortisol is the primary HPA hormone and it can be measured
Send us your draft and goals—our editors enhance clarity, fix errors, and keep your style. You’ll get a pro-level paper fast.
non-invasively and reliably in saliva (Helhammer, Wust, & Kudielka 2009;
Turner-Cobb, 2005; Granger & Kivlighan, 2003). When the body is stressed, the
HPA axis releases higher levels of cortisol resulting in metabolic imbalances
involving blood sugar and insulin, higher blood pressure, faster heart rate, mood
changes, thyroid imbalances and weakened immunological responses (Bruyere, 2009).
Yep! We’ll suggest ideas tailored to your field—engaging and manageable. Pick one, and we’ll build it into a killer paper.
A normal salivary cortisol stress reactivity response consists of a peak elevation
of salivary cortisol concentrations 10 minutes after the cessation of the test stressor
with a decrease to pre-stress levels approximately 90 minutes after the start of the test
(Kirschbaum, Pirke & Hellhammer, 1993). In addition, heart rates peak during the
protocol’s stressful task and then drops to baseline once the stressor stops (Kirschaum,
Pirke, & Hellhammer, 1993). In a recent study, prematurely born age 6 -10 years olds
were found to have an exaggerated cortisol response when faced with a social stressor
Yes! Need a quick fix? Our editors can polish your paper in hours—perfect for tight deadlines and top grades.
in a reliable laboratory paradigm, and more emotional and memory problems
(Quesada, Tristao, Pratesi & Wolf, 2014). Biological stress responses (i.e. cortisol)
play a reciprocating role whether the stress is physical or psychological.
Psychological stress (i.e. social evaluation and the perception of uncontrollability in
the situation) activates the cortisol response (HPA Axis), which in turn effects the
physical systems. Conversely physical stress activation (i.e. pain) of the cortisol
Sure! We’ll sketch an outline for your approval first, ensuring the paper’s direction is spot-on before we write.
system (HPA Axis) is associated with psychological changes in affective and
cognitive processes (Smith & Vale, 2006; Dickerson & Kemeny, 2004).
This study uses a standardized, widely used and well-researched laboratory test
for inducing moderate psychobiological stress responses called the Trier Social Stress
Test (TSST), (Kudielka, Hellhammer & Kirschaum, 2010; Kirschbaum, Pirke,
Hellhammer, 1993). In a meta-analysis of 208 laboratory stress studies, the TSST
was found to repeatedly induce changes in the concentration levels of cortisol (both
serum and saliva), as well as other major HPA Axis endocrines, and to significantly
Definitely! Our writers can include data analysis or visuals—charts, graphs—making your paper sharp and evidence-rich.
cause an increase in heart rate (Kirschaum, 2010; Kudielka, Hellhammer &
Kirschaum, 2010). Two key components of the TSST’s protocol are well studied and
known to be needed to induce a reliable and strong activation of the HPA Axis
measured in salivary cortisol. The components are the psychological stress of the
threat of social evaluation, and the perception of uncontrollability in the situation
(Kirschbaum, 2010; Dickerson & Kemeny, 2004). Over fifteen years of TSST
research has shown an increase by 50-300% over baseline in endocrine,
immunological and cardiovascular parameters (Kirschbaum, 2010).
Young adults born early with immature body systems may not just simply grow
out of it and catch up to those born full term (URI, 2011). Subtle, minor and clear
We’ve got it—each section delivered on time, cohesive and high-quality. We’ll manage the whole journey for you.
differences in attention, hyperactivity, and emotional and socialization effectiveness
have been found during childhood and adolescence (Healy, 2010). Guided by the
DOHaD theory, the developmental challenges of independent living at age 23 years
call for greater knowledge about how mechanisms of stress and capacity for response
are seen in former premature infants. There is minimal research on 23-year-old
Yes! UK, US, or Aussie standards—we’ll tailor your paper to fit your school’s norms perfectly.
outcomes of stress, coping, emotional intelligence, emotional health, stress reactivity
responses and the progression of emotional disorders. More knowledge about the
relationship of premature birth, the neuroendocrine stress response, self-reported
stress, coping and emotional intelligence will expand our understanding of the well
being of young adults and their attainment of developmental milestones. (Mannisto, et
If your assignment needs a writer with some niche know-how, we call it complex. For these, we tap into our pool of narrow-field specialists, who charge a bit more than our standard writers. That means we might add up to 20% to your original order price. Subjects like finance, architecture, engineering, IT, chemistry, physics, and a few others fall into this bucket—you’ll see a little note about it under the discipline field when you’re filling out the form. If you pick “Other” as your discipline, our support team will take a look too. If they think it’s tricky, that same 20% bump might apply. We’ll keep you in the loop either way!
al., 2015; Simpson, 2009; Tarasuik, et al., 2009).
Purpose
The Developmental Origins of Health and Disease (DOHaD) framework provides
the theoretical perspective for the proposed study. DOHaD asserts that early prenatal
Our writers come from all corners of the globe, and we’re picky about who we bring on board. They’ve passed tough tests in English and their subject areas, and we’ve checked their IDs to confirm they’ve got a master’s or PhD. Plus, we run training sessions on formatting and academic writing to keep their skills sharp. You’ll get to chat with your writer through a handy messenger on your personal order page. We’ll shoot you an email when new messages pop up, but it’s a good idea to swing by your page now and then so you don’t miss anything important from them.
and neonatal stress seen in HPA axis function affects later health and behavior. It
offers a mechanism to enable the understanding of salient young adult developmental
performance abilities. This is a secondary analysis of a well- characterized cohort of
premature infants categorized by neonatal illness into four groups of prematurely born
infants (Appendix A Measurements) and one group of full-term infants (for a total of
5 groups) who were assessed at age 23 years in a research protocol, which included
measures of stress, coping, emotional intelligence, emotional health and
the Trier Social Stress Test. The purpose of the study is to: 1. Compare the effect of
prematurity on stress, coping, emotional intelligence and emotional health at age 23
years. 2. Examine the neuroendocrine functioning of the stress response and
the stress recovery period at age 23 years. 3. Examine emotional health with HPA
Axis stress reactivity responses accommodating for prematurity and gender. The
knowledge gained from this study can help to inform how neonatal stress of
prematurity effects young adult coping, emotional intelligence, physiological
responses, developmental milestones and emotional health at age 23 years in a sample
at risk for HPA dysfunction. The results can help to identify who may be at risk, the
role of the neuroendocrine systems as an underlying mechanism, and suggest clinical
interventions to be taken to avoid risk factors and promote future adult health
outcomes (Rice, 2012; Kirschibaum. 2010; Sullivan, 2008).
Aims and Hypotheses
In a sample of young adults at age 23, former premature infants with a wide
variation in diagnoses of neonatal illnesses and a full term group, the aims of the
study, with related hypotheses are:
Aim 1. Compare the effect of prematurity on stress, coping, emotional
intelligence and emotional health.
Hypothesis 1. Higher self-reported stress scores, higher use of avoidance
coping types, lower emotional intelligence scores and more emotional health
disorders will be found for the adults at age 23 years born prematurely
compared to the term-born adults.
Aim 2. Compare the salivary cortisol response to social stress between premature
and term-born infants using stress paradigm of the Trier Social Stress Test
(TSST).
Hypothesis 2. Adults at age 23 who were born prematurely will have a
prolonged stress recovery period of the TSST.
Aim 3. Examine the relationship between effect of emotional health and on the
stress recovery period of the TSST measured in salivary cortisol.
Hypothesis 3. The stress recovery period for adults at age 23 years with
emotional health problems will be prolonged compared to adults without
emotional health problems when prematurity is controlled.
Summary
This study used a well-characterized, longitudinal sample of preterm and full term
born infants who have been followed from birth in a series of research studies. The
study used neonatal data and self-report of stress, coping and emotional intelligence,
clinical diagnosis of emotional health, and neuroendocrine function during a social
stress paradigm at age 23 years in a secondary analysis. The study is congruent with
the original, larger, study using the same theoretical framework and relevant variables
to examine self-reported stress, coping, emotional intelligence and emotional health
with the primary biomarker of HPA axis system, cortisol. The overall aim of the
study is to examine self-reports of important emerging adult independent function with
neuroendocrine activity in the well-standardized social stress test, the TSST. The
brain areas most affected by stress are the same areas involved in adapting to stress
and coping effectively (Compas, 2006). Researching these integrated
psychobiological processes through multiple analyses will lead to further
understanding of how stress effects young adults emotional development (Compas,
2006). This study has the potential to add relevant knowledge about salient
developmental characteristics, elements and competencies. The following chapter (2)
provides the scientific literature in support of this study. These include the DOHaD
theoretical framework and developmental milestones at age 23 years old of the
emerging adult who was prematurely born. The use of secondary longitudinal data
for analysis will also be addressed.
CHAPTER TWO
Theoretical Background and Related Literature
In this chapter, selected theoretical perspectives for this study are delineated,
specifically the Developmental Origins of Health and Disease (DOHaD),
neuroendocrine function of the HPA Axis, and prematurity. Age appropriate young
adult development at age 23 years will be described in relation to concepts of stress,
coping, emotional intelligence, and emotional health. Prematurity effects compared
to the full term born for 23 year olds will be understood within a disease
developmental theory integrating both biological and psychosocial aspects.
The discussion will begin with a historical review of the DOHaD theory and the
contributions up until present time. Included is a review of the construct development
of emotional intelligence and the relationship of DOHaD to stress, coping and
emotional health.
Theoretical Perspectives
The relatively new Developmental Origins of Health and Disease (DOHaD)
theory has gained scientific acceptance within the last thirty years (Wandhwa, Buss,
Entringer & Swanson, 2009). DOHaD postulates that fetal and neonatal stressors
affect the neurological and endocrine systems adaptive responses, specifically the
hypothalamic-pituitary-adrenal (HPA) axis, which is essential for physical and
psychological growth (Barker & Thornburg, 2013; Carpenter, Gawuga, Tyrka, Lee,
Anderson, & Price, 2010; Wandhwa, et al., 2009; McEwen, 2003; Sapolosy, 2001).
The major stress pathway of the neurological system is the HPA Axis (Figure 1)
which releases cortisol. Cortisol, the most dominant stress hormone that crosses the
blood – brain barrier, has the important function of adapting the body to both physical
and emotional stress responses (Bruyere, 2009). Additionally cortisol is vital in the
regulation of blood vessel tone, the inflammatory response, stimulation of glucose
production, insulin, and metabolism (Bruyere, 2009). HPA functioning is altered by
stress during structural growth periods resulting in permanent programming of early
life stress responses that contribute to disease formation later in life (Sullivan, Hawes,
Winchester & Miller, 2008).
Figure 1
Hypothalamic-Pituitary-Adrenal Axis
Figure 1. Reprint by permission from Worth Publishers. “An Introduction to Brain and Behavior (5th Ed.)” by Bryan Kolb and Ian Q. Whishaw, 2016. Copyright 2016 by Worth Publishers. From: AN INTRODUCTION TO BRAIN AND BEHAVIOR 5E, by Bryan Kolb, et al, Copyright 2016 by Worth Publishers. Used by Permission of the publisher.
Premature birth (<37 weeks gestation) occurs at a rate of one out of every nine
births, is the leading cause of infant deaths and long-term neurological disabilities in
children (CDC, 2014). The normal duration of pregnancy is 9 months (280 days)
with full term birth occurring at 40 weeks gestation (Taber’s, 2009). Preterm birth,
either naturally or by cesarean section, is “arbitrarily defined as before 37 weeks”
(WHO, 2015; Johansson & Cnattigius, 2010). Preterm birth can be further
subdivided into: moderately premature (32-<37 weeks), very premature (28-32
weeks), and extremely premature (<28 weeks), (WHO, 2015). The characteristics of
low birth weight and rates of fetal growth has also been used to define prematurity.
In preterm research studies, the combination of gestation weeks and birth weights are
used to avoid any misclassification especially with infants who have growth
restrictions (Johansson & Cnattigius, 2010). Low birth weight is <2500g (5 lbs. & 8
oz.), very low birth weight is <1500g (3 lbs. & 4 oz.), and extremely low birth weight
is <1000g (2 lbs. & 3 oz.), (Johansson & Cnattigius, 2010).
Surviving preterm born infants may have intellectual disabilities, neurological
problems, respiratory, visual, hearing and digestive problems (CDC, 2014; Martin &
Osterman, 2013). Premature infants have experienced prenatal stress, often from
health risk factors in the mother and postnatal stress from months–long intensive
care in the Neonatal Intensive Care Unit (NICU). These early stress experiences
evoke broad biological responses in the underdeveloped premature infant’s
neurophysiological systems including brain growth occurring during uterine
development (Phillips, 2001) and peak growth spurts well into the mid-twenties of
age (Epstein, 1986). Thus, the premature infant’s neuroendocrine system is
frequently activated leading to the inductive development and empirical evidence in
support of DOHaD theory.
Historical Evidence and Perspectives
DOHaD evolved from Barker’s original “Fetal Origins Hypothesis” which
originated inductively from epidemiological studies. (Barker, 1990; 2004, 2007;
Barker & Thornburg, 2013; Wandhwa, et al., 2009; Gluckman & Hanson, 2007;
Reynolds, 2007; Hofman, Regan & Cutfield, 2006). During this time period
multiple retrospective mortality and epidemiological studies from different countries
showed evidence that adult height and geographical differences were related to infant
mortality caused by heart disease (Barker, 1990, Barker, Erickson, Forsen, & Osmond,
2002; Phillips, 2001). An influential study, consisting of 499 people at age 50 born
in England, revealed their current blood pressure measurements and hypertensive risk
factors were strongly related to the measurements of their hospital-recorded placenta
and birth weights (Barker & Osmond, 1986; Barker, 1990). A lack of evidence was
found for the role of some commonly involved environmental variables in heart
disease, such as a high fat diet, and this finding prompted an alternative hypothesis
(Barker, 1995, 2007; Barker & Osmond, 1983). As a result of this landmark study, a
paradigm shift representing a new conceptualization of disease causation occurred
(Barker, 2007). This shift in scientific thinking about adult diseases, which was
defined as degenerative in nature and viewed as a result of gene and environmental
interactions, occurred and resulted in the inclusion of biological programming during
fetal and infant life (Barker, 1990) as a plausible explanation (Gordis, 2009).
Barker’s (1995) initial assumption was: “ fetal under-nutrition in middle to late
gestation, which leads to disproportionate fetal growth, programs later coronary
heart disease (p 171)” lead to further studies from this hypothesis. Later Barker
(2004) refined this to the hypothesis:
“Cardiovascular disease and type 2 diabetes originate through developmental
plasticity, in response to undernutrition. As it is now known that growth during
infancy and early childhood is also linked to later disease “developmental origins
hypothesis’ is now preferred (p. 114).”
Barker, defined a process of developmental plasticity as: “ a critical period when a
system is plastic and sensitive to the environment, followed by loss of plasticity and a
fixed functional capacity” (Barker, 2007, p 415). According to Barker, developmental
plasticity also has three features: 1. The response will depend on the nature of the
environmental cue. 2. There are critical time periods for different systems when
changes will occur and these changes may be temporary or permanent. 3. Duration of
these critical time periods are different depending on the structure with the brain
periods longer. These changes can be gross, substructure or functional.
The imbalance of fetal nutrients and oxygen was thought to result in an alteration
of not only metabolic yet endocrine functioning leading to smaller birth weights and a
variety of adult pathologies (Drake, Tang, & Nyirenda, 2007; Phillips, 2007; De Boo
& Harding, 2006, Gibson, Carney & Wales, 2006). Despite the scientific acceptance
of this explanation, methodological issues surrounding the use of body measurement,
birth weight or gestation age, and studies designed without a well-characterized cohort
utilizing prenatal and adult health outcomes, as well as observational and prospective
designs, added to concerns about confounding variables (socioeconomic status, diet,
cigarette smoking, physical exercise and selection bias), statistical effect sizes
(attrition and statistical over adjustments) and publication bias (Skogen & Overland,
2012; Erickson, 2006; Godfrey, 2006). A 2003 meta-analysis study addressing
publication bias relating to low birth weight and higher blood pressure found a weaker
association than initially determined yet maintained support for the fetal origins
hypothesis (Skogen & Overland, 2012). Despite a weaker association found, while
addressing some of the common confounding variables as alternative explanations,
better research methodologies resulted and improved the replication of findings
(Gordis, 2009).
Further studies from a variety of countries designed to control for confounding
variables supported the association between low birth weights as a fetal antecedent to
diseases (Barker & Bagby, 2005; Vohr, Wright, Dusick, Mele, Verter, Steichen,
Simon, Wilson, Broyles, Bauer, Delaney-Black, Yolton, Fleisher, Papile & Kaplan,
2000). At the same time debates occurred focusing on the idea that the only
important applicable time period for DOHaD was during pregnancy and the theory
was useful in explaining only cardiovascular diseases (Gluckman & Hanson, 2006;
Godfrey, 2006). Indeed, DOHaD flourished in explaining cardiovascular risk (Bryan
& Hindmarsh, 2006). Later, researchers significantly correlated low birth weight with
increased risk in a number of diseases that are part of the metabolic syndrome
(Hofman, Regan & Cutfield, 2006) such as truncal (middle body) obesity,
hypercholesterolemia, atherosclerosis, coronary artery disease, insulin resistant
diabetes mellitus, cardiomyopathy, congestive heart failure, autoimmune disease,
anxiety, depression, chronic pain and headache (Fricchione, 2015). Replicable cross
sectional studies of relationships between disease formations with metabolic illnesses
supported further study of the HPA axis associations.
The results from a retrospective longitudinal study of Helsinki, Finland male
adults, gave credence to the findings that smaller infants have a higher rate of
cardiovascular disease for men in adulthood (Ericksson, Forsen, Tuomilehto, Osmond
& Barker, 2001, Godfrey, 2006). The sample size consisted of 4,630 men born in
Helsinki (1934-44) and utilized child welfare clinic medical health records with
multiple time points of childhood through adult weight recordings, height
measurements and hospital admissions for coronary heart disease (Ericksson, et al.,
2001). Overall, low birth weight was associated with heart disease, low weight gain
was associated with an increased risk of heart disease and rapid weight gain after age 6
was associated with further risk (Ericksson, et al., 2001). As a result of this study,
determining what changes occurred in prenatal growth and those that occurred later
lead to focusing on the interactions of both prenatal and postnatal environments in the
development of adulthood cardiovascular diseases (Ericksson, 2006; Godfrey, 2006).
Concurrently animal researchers showed that exposure of rats during pregnancy
and after birthing, along with their offspring, to a variety of stressors resulted in
elevated stress-induced cortisol levels in the off-spring and disease development
(Phillips, 2001). This study added a “dose-response” relationship, or intensity and
timing of the exposure of stressors to the DOHaD research literature. Animal studies,
pinpointed the HPA Axis response to stressors introduced during critical times of rat
brain growth, that occurred after birth and produced permanent changes in the animals
HPA Axis response (Matthew, 2002; Phillips, 2001). As mentioned earlier, in
humans, critical brain growth occurs during uterine development (Phillips, 2001) and
continues with peak growth spurts well into the mid-twenties of age (Epstein, 1986).
Sterling and Eyer in 1988 coined the word “allostasis” (Sterling & Schulkin,
2004) based on research with monkeys while studying high blood pressure. Allostasis
was now a new paradigm to explain arousal pathology and replaced homeostasis
conceptually. Allostasis involves regulation by: varying parameters and variations in
anticipated demands. A new core assumption now was that physiology is sensitive to
social relations. Allostasis also depended on higher-level brain functioning, other
then basic physiological automatic responses, and involved prefrontal cortex
regulation. Anticipatory regulation for anxiety and satisfaction was found to rely on
the prefrontal cortex through neuronal mechanisms.
McEwen, in 1989, further developed these principles through “allostatic load” and
is credited with the advancement of the theory by publishing research findings related
to human autonomic, central nervous system, endocrine and immune system activity
(Sterling & Schulkin, 2004). McEwen (2006) implicated stress to an event as an
individual biological response factor in the development of a disease. In addition to
acute stress events, McEwen defined the effects of general “wear and tear” (p 367) on
the body as allostatic load that targets the HPA Axis, releasing an end product of
cortisol and can lead to the development of adulthood diseases (McEwen, 2003 &
2006).
The main hypothesis of the DOHaD theory, involves one sensitive brain area of
prenatal and postnatal development occurring in adulthood disease development by
resetting the glucocorticoid endocrines, which is the Hypothalamic-Pituitary –Adrenal
(HPA) Axis (Sloboda, Newnham, Moss and Challis, 2006). McEwen (2008) further
delineated this dimension of the theory by postulating that stress hormones have a
central effect in health and disease by providing protective, damaging and mediating
effects.
These mediating stress effects can be from a physical, psychological, emotional,
cognitive, intellectual, major life events, environmental or social/caring interactions.
Biologically, individuals can either adapt to acute stress (allostasis) or become
overloaded (allostatic load) with chronic stress resulting in pathophysiological changes
(McEwen & Seeman, 2006). See Figure 2.
Figure 2
Stress Response and Development of Allostatic Load
Figure 2. Reprinted by permission from Macmillan Publishers Ltd;
Neuropsychopharmacology, 2000, by B., McEwen, Allostasis and allostatic load: Implications for neuropsychopharmacology, Neuropsychopharmacology, 22, 108-124. Copyright 2000 by Nature Publishing Group.
The brain is viewed as not only the controller of the stress response yet conversely
as the target (Rubinow, 2006). The HPA Axis as programmed is effected by the
totality of lifelong stressors (cumulative risk) and negative effects on the brain and
body (allostasis/allostatic load) leading to the long-term consequences of adulthood
disease (Manzanares, Monseny, Ortega, Montalvo, Franch, Gutierrez-Zotes,
Reynolds, Walker, Vilella & Labad, 2014; McEwen, 2012, Sullivan, et al., 2008). In
other words, the adaptability to a stressor or anxiety rather than the initial reaction will
predict long-term outcomes and allostatic load becomes the unifying concept between
cumulative risk and HPA dysregulation (Manzanares, et al, 2014; McEwen, 2012,
Sullivan, et al., 2008).
McEwen did initially base his theory on the idea of homeostasis, which
conceptually is a bodily system that is stable and unchanging (Dictionary.com, 2015)
and postulated there is an optimal level and ideal set point (McEwen, 2004). This
explanation evolved to include the idea of variation (allo) of levels and set points
achieving a balance in the total system (Dictionary.com, 2015). McEwen points out:
Homeostasis is about adjusting this level while allostasis is about the brain
coordinating body-wide changes to achieve stability through change (McEwen, 1998
& 2004). Thus adaptation in a central concept of the theory. Stressors, according to
McEwen result in experiences that are either acute or chronic. Acute stress is the
“fight or flight” response or those responses resulting from major life events. Chronic
stress is defined as the accumulation of minor and daily stresses.
There are four types of allostatic load (Figure 3): normal, repeated, lack of
adaptation and inadequate (McEwen, 2000 & 2007). Endocrine and metabolic
Figure 3
Four Types of Allostatic Load
“Four types of allostatic load are illustrated. The top panel illustrates the normal allostatic response, in which a response is initiated by a stressor, sustained for an appropriate interval, and then turned off. The remaining panels illustrate four conditions that lead to allostatic load: 1) Repeated “hits” from multiple novel stressors; 2) Lack of adaptation; 3) Prolonged response due to delayed shut down; and 4) inadequate response that leads to compensatory hyperactivity of other mediators, e.g., inadequate secretion of glucocorticoid, resulting in increased levels of cytokines that are normally counter-regulated by glucocorticoids). Figure drawn by Dr. Firdaus Dhabhar, Rockefeller University.”
Figure 3. Reprinted by permission from Macmillan Publishers Ltd; Neuropsychopharmacology, 2000, by B., McEwen, Allostasis and allostatic load: Implications for neuropsychopharmacology, Neuropsychopharmacology, 22, 108-124.
Copyright 2000 by Nature Publishing Group.
responses protect the body from allostatic load in the short term through homeostatic
adaptation called allostasis. Chronic stressors or allostatic load, whether physical,
psychological or a combination, result in structural brain changes that effect our
physiological and behavioral responses and lead to the development of adulthood
diseases (Ewen, 2003 & 2006).
The stress experience or the stress response that the individual has to a potential
stressor, is the focal point (McEwen, 1998) and added to “Barker hypothesis” of
prenatal stage development, the future time determinants of adulthood diseases
(Skogen & Overland, 2012). Stress as defined by McEwen is a “state of real or
perceived threat to homeostasis” and stressors are “aversive stimuli” while
“maintaining homeostasis through activation of complex responses involving the
endocrine, nervous and immune system” is the stress response (McEwen, 2006).
Luthar, Cicchetti and Becker, 2000, are clearer in their definition of the stress
response, as a dynamic equilibrium, meaning an ability to sway and not as a fixed or
static state. When a good adjustment is achieved across different domains of the
stress response, in the face of significant adversity, then “resiliency” is achieved
(Luthar, Cicchetti & Becker, 2000; Ficchione, 2015). Thus, the capacity to maintain
allostasis while challenged by mental and physical aversive stimuli to well being,
constitutes resiliency (Ficchione, 2015). One Mind Body Medicine equation
(hypothesis) is formulated as (Ficchione, 2015):
Stress (Allostatic Loading) = Selective Vulnerability: Propensity to physical and
Resiliency Factors mental illness
Ficchione (2015) defines resiliency factors as: “relaxation response, mindfulness;
social support/prosociality; cognitive skills; positive psychology; spirituality;
exercise; nutrition; healthy habits”.
According to McEwen (1998) there are two factors that determine the individuals
stress response: how the situation is perceived and the individuals’ general state of
health (determined by genetics, behavior and lifestyle choice), (See Figure 2).
Matthews (2002) added that the timing and intensity of the aversive event and/or an
intervention also effects HPA axis development and functioning. This focus on later
stress experiences added environmental triggers to critical or sensitive growth time
periods as a second possible causal pathway to disease suggesting the involvement of
more than one critical time period (Skogen & Overlad, 2012). Stressors, occurring
prenatally result in adaptive changes within the HPA-Axis, become permanently
programmed, and impact health during adult life (Reynolds, 2013; Sullivan, Hawes,
Winchester & Miller, 2008; Barker, 2007) while later environmental triggers and
responses add to the allostatic load depending on coordination with sensitive growth
time periods (Skogen & Overland, 2012).
The body’s stress response helps individuals adapt to a problem and marshal the
resources to respond which includes releasing response coordinating hormones. A
unifying and central relationship is if the stress response is activated too frequently or
under utilized then the stress-response itself can be more harmful than the stressor and
this concept is called allostatic load (McEwen, 1998 & 2004). There has been
controversy over the labeling of this phenomenon yet the underlying concept has not
been challenged. McEwen (2004) does identify features of some stress processes that
do not change in order to help and adds those processes that do vary in the context of
life cycles, individual experience and responses to the physical and social environment
(McEwen & Wingfield, 2010). The challenge, according to McEwen, in the
definition is that allostasis adds to homeostasis a focus on how individuals have access
to bodily resources to respond to problems with the environment (McEwen, 2004).
Welberg and Seckl, 2001, found that stress during pregnancy could permanently
alter behavioral and/or physiological reactivity to stressors (Sullivan, et al, 2008).
The authors extensively reviewed available research of epidemiological, animal
biological, human biological, anxiety, cognition, neural mechanisms, under-nutrition,
interactions with postnatal environments and glucocorticoid studies. In terms of HPA
function, the evidence showed:
“Birth weight correlates closely with HPA measures from infancy (206), through
adolescence and young adulthood (207) to old age (208). These data suggest that
low birth weight associates with both increased basal and ACTH-stimulated
cortisol levels (207, 209). Taken as a whole, these findings are compatible with
the hypothesis that fetal overexposure to glucocorticoids whether exogenous DEX
or endogenous cortisol may underlie at least in part the connection between the
prenatal environment and adult stress-related and behavioral disorders (Welberg
& Secki, 2001, p 123).”
As this evidence became available another shift in thinking about adulthood
disease formation occurred and became widely accepted by the scientific community
(Skogen & Overland, 2012; Salonen, Kajantie, Osmond, Forsen, Yliharsila, Paile-
Hyvarinen, Arker & Eriksson, 2011; Gluckman & Hanson, 2006; Godfrey, 2006).
The scientific community was now in consensus that relevant life periods are on a
continuum that includes during pregnancy, infancy and throughout the life span
(Gluckman & Hanson, 2006; Godfrey, 2006). The focus of the theory was now
based on two main assumptions. The first assumption is early life events that occur
during periods of critical biological growth partially determine future adulthood
disease development and secondly, this has implications for both disease development
and promotion of health (Gluckman & Hanson, 2006; Godfrey, 2006). DOHaD
theory research then branched into three major areas of interest: 1. Maternal, fetal and
postnatal nutrition, 2. Preterm birth and, 3. Epigenetics (or gene modification),
(Wadhwa, et al., 2009; Waterland & Michels, 2007).
DOHaD theory has been applied to a variety of diseases and health concerns:
behavioral, cancer, cognitive, diabetes, metabolic, muscular, neurological,
psychological and respiratory (Barker & Thornburg, 2013; Gluckman & Hanson,
2007; Hofman, Regan & Cutfield, 2006; Barker, 2005 & 2004). The theory is widely
used in behavioral medicine and specifically with interventions directed at reducing
stress responses (Benson, 2015). Researchers are also exploring the effects of
stressors, as measured by cortisol levels and magnetic resonance imaging, with major
psychiatric disorders such as post-traumatic stress disorders, anxiety responses, stress
responses, cognitive functioning, eating disorders, childhood disorders, personality,
long-term effects of child abuse, psychosis and addictions (Nosarti, Murray & Hack,
2010). Indeed, anxiety, an autonomic nervous system response triggered by HPA
functioning, is a general symptom of stress and co-occurs with other psychiatric
disorders, especially depressive disorders (APA, 2000).
Theory Analysis
DOHaD a relatively new theory addressing the origins of adulthood disease is
widely accepted, utilized in clinical interventions and research studies. Originating
from epidemiological study results DOHaD has developed into a major disease
causation theory. The original theory was intended to explain one aspect of disease
causality and to be applicable to multiple diseases including those “future entitles yet
unknown” (Barker, 2007). Extending the original Fetal Origins Hypothesis, beyond
the initial hypothesis of environmental influences during pregnancy has an effect on
later development, expanded the perspective beyond biological determinism (Skogen
& Overland, 2013). The addition of stress responses through further refinement of
the HPA Axis dysregulation hypothesis, multiple critical time periods and life span
influences took into consideration the role of other causal issues. In addition to
physical stressors, an individual’s perception of stress as threatening or uncontrollable
has been shown to activate the HPA axis as well as coping styles choices affects on
later life stress-related disease development (Figure 4). The continued development
along this thinking moved DOHaD to a fuller life course perspective with multiple
causal factors including emotional health (individual perceptions of stress interpreted
as threatening or not) environmental (such as parenting) and for some the addition of
the biological bases of mammalian evolutionary attachment (social influences)
perspectives (Skogen & Overland, 2013; Fricchione, 2011).
DOHaD theory defines a plausible biological temporal relationship between
disease formation and the role of the HPA axis. Research results show an association,
of a dose-response relationship of intensity and timing of stressors, and replication of
Figure 4
The Cardiovascular Toll of Stress (Emotional and Physical Stressors, HPA Axis &
Health)
Figure 4. Reproduced with permission of Lancet Publishing Group; Brotman, D.J., Golden, S. H., & Wittstein, I.S. (2007) The cardiovascular toll of stress, The Lancet,
370, 1089a1100.
findings in specificity to stress-related illness, although the majority of research
in the United States, has been at discrete time periods in a person or population’s life.
DOHaD theory states the necessary condition of structural and functional changes
prenatally and whether any of this is irreversible remains to be seen (Skogen &
Overland, 2012). Some common confounding variables as alternative explanations
have been addressed and the national government (National Institute of Health) has
prioritized the use of longitudinal studies to address the complexities of what factors
(NIHR, 2015), may or may not be sufficient or necessary for disorders.
Literature recommendations for further research focus on utilizing regression
modeling statistical strategies to address: the association between the two variables of
early exposure and adult outcomes, intermediate exposures, the interaction between
the early exposure and intermediate variables and to what degree the intermediate
variable is related to disease outcome (Skogen & Overland, 2012). Research into the
effects of stress experiences on HPA Axis development, function and dysregulation
also requires addressing the roles of birth term, gender and social inequalities as
confounding moderating variables (Matthew, 2002; Sapolsky, 2009). The renewed
interest in DOHaD theory is leading researchers into areas of study that promise to
identify risks and protective mechanisms; locate periods of transitions into pathology,
develop preventive and possibly corrective interventions to intervene in the
progression of disease pathologies over the course of a lifetime (McEwen &
Wingfield, 2002; Sullivan, Hawes, Winchester & Miller, 2008; Ben-Sholmo & Kuh,
2002).
Socioeconomic Status (SES)
Many socioeconomic status (SES) factors are associated with low birth weight,
coronary heart disease, under nutrition, low literacy rates and health disparities
(Senterfitt, Long, Shih, & Teutsch 2013; Baber, Muzaffer, Khan, Imdad, 2010).
Social and economic factors are considered the largest single predictor of health
outcomes and influencer of health behaviors (Senterfitt, et al., 2013). Disparities
between countries in preterm birth weights have been partly explained by differences
in SES (Johansson & Cnattigus, 2010). Multiple studies have found that the lower
the social, education, and economic position the higher the unhealthy behaviors (i.e.,
smoking, physical inactivity) and inability to engage in healthy behaviors (Senterfitt,
et al., 2013).
The World Health Organization (WHO, 2015) includes determinants of SES
consisting of: the physical environment, the person’s individual characteristics and
behaviors (including how they “deal with life’s stresses and challenge, (p 1)”, social
support networks, genetics, available health services and gender. Additionally, a
WHO (2003) sponsored study, found middle-class office workers and lower ranking
staff has more disease and die earlier than higher positioned workers. The WHO
report (Wilkinson & Marmot, 2003) focuses on ten main areas of what is known:
1. Life expectancy and shorter life spans occur further down the social ladder.
2. Stressful circumstances lead to worry, anxiety, inability to cope that is damaging to
health. 3. Foundations are laid in childhood: “slow growth and poor emotional
support raise the lifetime risk of poor physical health and reduce physical, cognitive
and emotional function in adulthood, (p 14)”. 4. Poor life quality shortens lives.
5. Stressful workplaces increase the risk of disease. 6. Health risks of
unemployment increases the rates of premature death. 7. Supportive relationships
contribute to health. 8. Individuals addictions to alcohol, drugs and tobacco numb
difficult conditions and lead to downward mobility. 9. Healthy food is a political
issue. 10. People’s dependence on cars has increased resulting in less walking and
social contact and more traffic accidents and air pollution.
One of the earliest criticisms of the interpretations from DOHaD studies is the
the confounder of SES could explain results used to support the theory (James,
Nelson, Ralph, & Leather, 1997; Skogen & Overland, 2012). James, et al, (1997)
found lower socio- economic groups have more premature and low weight births,
more illnesses, more risk factors and less nutritional diets. The DOHaD theory
emphasizes that chronic exposure to stress mediators of the HPA Axis and the
sympathetic nervous system effects multiple organs resulting in disease (Dowd,
Simanek & Alello, 2009) although SES confounding variables in earlier studies were
not adequately controlled or interpreted.
Allostatic load has been used to explain part of the association between SES,
health and disease. Lupien, King, Meaney, & McEwen (2001), as one goal of three,
explored the possibility that because lower SES status involved higher stress and
fewer coping resources then morning salivary cortisol levels would differ from other
SES groups. The cross-sectional experimental design study, utilized 307 children
from a school setting, with 6 age groups (6-16 years old) and two categories (low and
high) of SES. Overall findings showed that lower SES in children related to higher
cortisol levels with the impact of SES on cortisol absent after transition to high school.
The authors identified four possible social explanatory factors of: changing status,
influence of peers, influence of youth culture, and resilience.
In contrast a systematic review of the literature, extending up until June of 2009,
on SES and biomarkers of physiological systems, was conducted by Dowd, et al.,
(2009) to address SES, cortisol levels and indirect measures of allostatic load. A total
of 26 studies met the inclusion criteria of reported associations between an indicator of
SES and cortisol, and/or allostatic load. Fourteen of these studies utilized salivary
cortisol secretions. The findings overall were mixed with little evidence that lower
cortisol related to lower SES and lower SES related to higher allostatic load
measurements. Overall, the authors found more studies with no associations of
cortisol to SES than the intuitive finding of lower SES associated with higher cortisol
levels. The unexpected findings were attributed to differences in the nature of this
relationship or inconstancies in measurements and analysis of both cortisol and SES.
Standardization of cortisol procedures and analysis, variations in SES indicators used,
and the exclusion of subjects using stimulators of cortisol such as smoking, were
major recommendations for future research. Although the review focused on cortisol
level daily patterns and indirect measurements of allostatic load, both laboratory stress
induced and dexamethasone challenges, were felt to provide more controls for
research on the differences of SES on HPA function.
Pluobidis, Benova, Grundy & Layton, 2014, identified four major hypotheses
from the literature about the associations between SES and later life health: 1. Early
life SES directly effects later life health. 2. Early life SES indirectly effects later life
SES. 3. Early life and later life SES effects health through accumulation of risk.
4. Early life health indirectly effects later life health via later life SES. A sample of
aged 50-53 years was taken from an English longitudinal study on aging. Multiple
measurements of early life and later life SES, health, and fibrinogen levels (indicator
of aging) were obtained. The four major hypotheses were compared through
statistical modeling. In general, results found early life SES extends directly until the
beginning of old age and predicts health at age 65 and older yet fibrinogen levels will
vary.
Co-existing with SES are social risk factors defined as (Msall, Sullivan & Park,
2010): “suboptimal home and community environment, poverty, domestic violence,
drug addictions, crime, hunger, and poor quality housing (p 224).” The conditions
of low SES along with access to care issues, coping with multiple adversities,
helplessness and low self-esteem; contribute to the risk of preterm births (p 225)
along with ethnicity, family history, maternal characteristics, multiple pregnancies and
air pollution (Johansson & Cnattigius, 2010; Msall, Sullivan & Park, 2010).
Low SES is consistently associated with poor health and disease yet how this gets
translated into biological risk is uncertain and studies have shown inconsistent and at
time weak results (Pluobidis, Benova, Grundy & Layton, 2014; Senterfitt, Long, Shih,
& Teutsch 2013; Baber, Muzaffer, Khan, Imdad, 2010; Dowd, Simanek & Alello,
2009; Wilkinson & Marmot, 2003; Lupien, King, Meaney, & McEwen, 2001).
Methodological issues in past studies have helped confound the influence of SES and
effected some interpretations of DOHaD theory evidence.
In this study, participants’ selection criteria at birth, as designed in the original
research, involved representation from all SES groups in each variable of birth
status (preterm and full-term born) to control for this effect. Additionally later SES
status at age 23 was assessed for possible individual differences and SES group
variations from the prenatal time period. Multiple measures of SES status, in addition
to income, were used and included standardized instruments, education level,
occupation level categorization and neighborhood ratings (Farrington, 1991).
Race and Ethnicity
The Center for Disease Control (CDC) found differences in preterm birth by race
and ethnicity and statistically analyzed the relevant differences, using percentages, and
z tests at the 95% confidence level (Martin & Osterman, 2013). The percentage
results were: 1. Black infant preterm birth rate (17.1%) was 60% higher than for
White infants (10.8%). American Indian/Alaska Native (13.6%) and Hispanic
(11.8%) preterm birth rates were higher than White infants. 2. Black infants had
double the early preterm birth rate (6.1%) than Whites, 25% higher than Hispanics
(Reagan & Salsberry, 2005), and other ethnicities (2.9%). 3. Black infants were
40% “more likely to be born late preterm than White infants with Hispanic infants
more often than White infants, (Martins & Osterman, 2013).”
Reagen and Salsberry (2005) studied the health disparities of preterm births
among Blacks, Hispanics, and Whites focusing on social contexts of neighborhood
disadvantage and cumulative exposure to income inequality while controlling for
individual risk factors. Neighborhood poverty and housing vacancy rates increased
the rates of premature births for Blacks while income inequality directly effected only
Hispanics (Reagan & Salsberry, 2005). Not withstanding these findings, the close
relationship of social risk factors from low SES to ethnicity (Msall, Sullivan & Park,
2010) confounds the separation of SES from ethnicity effects. Likewise, other
epidemiological studies have shown, that among the multiple causes for spontaneous
preterm births, being a member of the Black race, is also a risk factor (Goldberg,
Culhane, Iams & Romero, 2008).
Mustillo, Krieger, Gunderson, et al., 2004, found self-reported experiences of
racial discrimination by Black women were related to premature birth weights and
may contribute to disparities in perinatal health between races (Black 50%: White
5%). One landmark study accounting for social disparities, showed that even college
educated Black women have an increase rate of premature births when compared to
White college educated women (Schoendorf, Hogue, Klieinman, et al., 1992). In past
racial and ethnic disparities research, studies have separated their focus on either the
social construct of race or the biological processes (Kramer & Hogue, 2009).
A systematic review of the research literature, in 2009, focused on integrating the
racial biological and social patterning of premature births, with the expressed purpose
of ‘understanding the etiology of black-white racial disparities in preterm birth
(Kramer & Hogue, 2009, p 85)”. Over 1,459 citations were reviewed spanning from
1960-2009. Studies utilizing ultrasound-based measurements and data cleaning
methodology approaches that decreased misclassification were utilized. Conceptual
framework reviews lead to 3 primary biological pathways mediating the racial
disparities in preterm birth: placental dysfunction, HPA dysfunction and
maternal-fetalinflammation. Pre and peri-conceptual maternal health as well as
genetic and epigenic pathways studies were included in the review. Overall the
researchers found evidence to support socially patterned maternal stress as a cause of
racial disparities. The identification of few studies addressing genetics and the
challenges of controlling for multiple causal explanations prompted the authors’
suggestions for future research. The suggestions included incorporating biological
markers into socially focused preterm birth studies as well as improved
epidemiological design studies.
In this secondary analysis longitudinal study, the original racial and ethnic
composition of the sampling is predominately White and reflective of the population
and geographical location in Southeastern New England from 1985 to 1989 (Sullivan,
et al., 2008). The homogenous composition of this study population will be
applicable to the White racial group and not reflect the disparities inherent between
Black and Hispanic populations. The identification of the White racial group preterm
health outcomes from 1985-1989 may contribute to further knowledge of health
advances made since that time period and could possibly be utilized to compare the
associated magnitude of racial disparities today.
Gender
Globally, males are slightly more likely to be born prematurely than females
(Katz, Lee, Kozuki, et al, 2013). Decades of past research have shown males born
prematurely have higher mortality and morbidity and the phenomena is often referred
to as “male disadvantage” (Brothwood, Wolke, Gamsu, Benson & Cooper, 1986;
Stevenson, Verter, Fanaroff, et al., 2000; Banga, Barche, Singh, Sheehan &
Vasylyeva, 2015). The confirmed risks of high blood pressure and placenta
abnormalities to the pregnant mother carrying a male fetus is thought to occur
secondary to sex differentiation hormones in utero and at conception (Katz, Lee,
Kozuki, et al., 2013, Ingemarsson, 2003). Moreover, Sweden national figures show
death rates are higher for males by 55- 60% when born between 23 and 32 gestational
weeks (Ingemarsson, 2003). Immediate complications of respiratory distress
syndrome are greater for prematurely born males and cognitive recovery after
intracranial hemorrhage is less when compared to premature females (Imaemarsson,
2003). Similarly, in the United States, males are also more likely than females
(OR = 1.21; 95% CI: 1.02 – 1.42) to be born at 33 to 36 weeks (McGregor, Leff,
Orleans & Baron, 1992). To put it another way, if a male and female are born at
the same prematurely gestational age then male infants risk becoming more seriously
ill than females (SMFM, 2015).
While prematurity survival rates have increased, the prematurely born at 25 weeks
will develop disabilities (1:10) such as lung disease, cerebral palsy, blindness or
deafness; 50% disabilities; and more commonly cognitive and neurological
impairments (Banga, Barche, Singh, Sheehan & Vasylyeva, 2015). A retrospective
chart review of 160 (male 59% and female 41%) pediatric records at a Texas clinic
focused on children and adolescents born prematurely and any gender differences in
medical diagnoses. The sample consisted primarily of White (39.2%) and Hispanic
(38.0%) races born prematurely and between 10 and 21 years old at the time of the
chart review. Gestational ages were divided into two groups of 32-37 weeks and
< 32 weeks with birth weight divided into 7 groupings ranging from extremely low
birth weight to large for gestational age. The incidence of neonatal complications
between genders was assessed according to: jaundice, metabolic complications,
respiratory distress syndrome, sepsis, intracranial hemorrhage and hypertension.
Long-term morbidities included ICD-9 diagnoses of: asthma, allergic rhinitis, cardiac
defects, behavioral issues, developmental delays, growth delay and kidney anomaly
and diseases. Even though, more preterm born males were at weights appropriate for
their gestational age, the study found males had a higher incidence of neonate
complications especially: jaundice (63.1 vs. 36.8%; p = 0.02), metabolic issues
(64.2% vs. 35.7%, p = 0 .03), and respiratory distress syndrome (60.5% vs. 39.4%,
p = 0.02), (Banga, Barche, Singh, et al., 2015). In contrast, prematurely born
females weights were primarily small for gestational age. No differentiation between
genders for neonatal diagnoses of intracranial hemorrhage, sepsis or hypertension
were identified. The only significant gender difference in long-term morbidities
found was notably in behavioral issues for males and mostly diagnosed with attention
deficit hyperactivity disorder (6% vs. 2%; p < 0.01), (Banga, Barche, Singh, et al.,
2015).
The prematurely born female chances of survival are higher than males yet Black
prematurely born females, weighing about 2.2 pounds or less, have a higher rate of
survival than their White peers (UF, 2006). Researchers (UF, 2006) who studied
vital statistics from Florida, between the years of 1996 and 2000 utilizing records of
5,076 babies born in the state, found females at lower birth rates faired better with
Black females fairing better overall. Although the researchers are yet unable to
explain why this racial and gender phenomena exists it is known that female
premature babies in general have more developed lungs than males (UF, 2006).
Finally, there are a few decades of history of the vulnerability of preterm males
over preterm females for increased mortality and morbidity. Studies have shown
despite advancements in preterm neonate care this phenomenon continues to exist as a
risk to full term pregnancy and neonatal complications with male births. A few
endocrine and biological adaptation explanations have been proposed without any
known etiology of this gender-related health disparity (Banga, Barche, Singh, et al.,
2015). In this study, overall gender differences as well as gender and birth status
interaction are analyzed to identify the direction and strength of this effect (Baron
& Kenny, 1986).
Prematurity and Development at Age 23 as Emerging Adults
Multiple factors including SES, race, gender, environment and lifestyles, to
mention a few, influence the health and the formation of physical diseases and
emotional health in all adults. The prematurely born Age 23 emerging adult
entered this world with the disadvantage of multiple immature bodily systems.
Additionally, as has been previously stated, human brain growth occurs during uterine
development (Phillips, 2007), the newborn’s central nervous system (CNS) evolves
rapidly and peak growth spurts continue well into the mid-twenties of age (Epstein,
1986) resulting in multiple sensitive time periods of critical influence. In preterm
infants who require extensive neonatal intensive care, it is possible that the HPA Axis
is repeatedly activated which may result in permanent programming of early life
responses (Maniam, Antoniadis, & Morris, 2014; Reynolds, 2013; Sullivan, Hawes,
Winchester & Miller, 2008). Routine medical procedures activate the newborns
stress response system to react and moderate levels of endocrine hormones have been
found (Jensen, Beijers, Riksen-Walravan & de Weerth, 2010) that contributes to
alterations within the HPA Axis or fetal programing from cell death, and failed or
delayed responses of the central nervous system (CNS), (Sullivan, Hawes, Winchester
& Miller, 2008). See Figure 5
Figure 5
Prematurity, Postnatal Stress and HPA Function
Figure 5. Reprinted by permission Mary. C. Sullivan. 2008-2013. In “Risk and
protection in trajectories of preterm infants: Birth to adulthood (Grant # NIH R01
NR003695-14).” Bethesda, MD, National Institutes of Health, National Institute of
Nursing Research.
Structural differences in the brains of premature low birth weight infants with
alterations continuing into adulthood have been found by researchers (Nostarti,
Murray & Hack, 2012). Measurements of brain pathology using a variety of
biomarkers, such as salivary cortisol levels as an endocrine marker of the HPA Axis
activation is in wide use and may serve as a transitional marker for psychological
pathology (Turner-Cobb, 2005).
Feldman, Weller, Sirota & Eidelman (2002) in Israel, studied the effects of
mother to infant (or Kangaroo Care) skin-to-skin contact on both prematurely and
full term born infants. Specifically they examined “infants’ capacity to regulate sleep
and wake states, organize behavior, regulate negative emotions, modulate arousal,
coordinate attention to mother and an object, and sustain effortful exploration of the
environment (p 194)”. The infants born prematurely showed an abnormal response
to stimuli and often could not inhibit reactions. Three theoretical perspectives were
included: There is unique time windows for input required for optimal development
of the central nervous system and behavioral organization. Sensory development is
sequential and lastly maternal proximity organizes sleep, rest and behavior inhibition.
A prematurely born group with intervention (n = 73) and a matched control group
(n = 73) without intervention was used. Pre and post interventions as well as
multiple time point measurements were used. The premature infants who received
skin-to-skin contact from the mother were found to benefit by improved behavior
organization and emotional regulation when they reached full term. Hence, self
regulation and the ability to adjust behaviors to the situation is a challenge to the
preterm infant, requires environmental control and sets up regulation parameters
overtime (M.C. Sullivan, personal communication, November 11, 2014).
Affect regulation of emotional experiences to serve a purpose or goal
contribute to meeting developmental milestones and adult maturation while emotional
influences on decision-making have been found during adolescent to contribute to
behavioral (alcohol and nicotine dependence), emotional and clinical disorders (Dahl,
2001). Prematurely born children are at increased risk for behavioral and emotional
health problems along with associated psychiatric disorders especially anxiety,
depression, inattention and social difficulties (Johnson & Marlow, 2011;
Strang-Karlsson, 2011). Children born at extreme prematurity have been found to
experience a 50-70% higher rate of attention and behavioral problems in school
despite normal IQ scores (Lynn, Cuskelly, O’Callaghan & Gray, 2011). Even
children born near term (34-35 weeks gestation) have a 36% increased risk for
developmental delay or disability at kindergarten age (Rabin, 2009). Preterm born
17-year-old late adolescents have a higher percentage of psychological problems
when compared to the United States national age-related statistics (NIMH, 2007a &
2007b; ADAA, 2007): 11% with ADHD compared to 3-5%; 12.1 % diagnosed with
depression compared to 5%; 9.8% diagnosed with anxiety disorders compared to
3.1% (Sullivan, 2008). Thus, prematurity is associated with behavioral and
emotional health issues, as well as, psychiatric disorders from preschool through
adolescence age, and have risk for continued problems in adulthood.
Miller, Sullivan, Hawes & Marks (2009), reported on their prospective,
longitudinal sample of 186 children, at age 12, grouped into four preterm perinatal
morbidity groups (healthy preterm without medical or neurological illness, medical
preterm with clinical illness but without neurological abnormality, neurological
preterm with severe illness and small for gestational age preterm with or without
medical problems) and healthy full-term comparison group. A variety of biological,
social and physical environmental factors were measured utilizing a battery of tests
and neonatal medical data sources. Differences for neurological status, motor status
and health at age 12 were significant with abnormal high rates in the four preterm
groups compared to the full term group. Total health outcomes of the four preterm
groups were 3.4 times more likely than term births to have overall abnormal health
status at age 12.
A secondary analysis of this data (Wright & Sullivan, 2011) demonstrated that
prematurity measured by birth weight was associated with childhood psychiatric
symptoms at age 12. Additionally, the mother’s perception of their premature child’s
vulnerability and psychiatric symptoms correlated positively at ages 4, 8, and 12.
Sullivan, Msall & Miller, (2012), found a higher percentage than the United
States’ statistics for psychological problems in their age 17 cohort of the study related
to attention deficit hyperactive disorder (ADHD), depression and anxiety. This
prospective study reported on the same cohort at age 17 consisting of 215 infants born
between 1985-1989 with preterm birth weights <1850 grams and grouped by neonatal
morbidity then compared them with a full term group. Outcomes of functioning and
disability included body functions, body structures, activities and participation.
Contextual factors were identified according to the World Health Organization
International Classification of Functioning (The ICF Model, WHO, 2002). At age 17,
180 of the 215 adolescents, completed the standardized assessment process that
analyzed health, neurological, chronic conditions, psychological, environmental-
socioeconomic, personal-neonatal morbidity and gender status. Overall results
indicated that physical long-term effects of prematurity were not only confined to
infants with very low or extremely low birth weight but also included small for
gestational age and preterm infants without neonatal complications. Higher
percentages of psychological problems, 11% ADHD (4.1%), 12.1% (5-8%)
depression, and 9.8% (3.1%) anxiety disorders were found.
Emerging Adults
The age period between 18-25 years old is now termed the period of “emerging
adulthood” due to cultural delays in reaching developmental milestones (Arnett,
2013). In the past, these ages were considered part of young adulthood, when the
taking on of adult roles were not delayed. Emerging adulthood, is now a separate
category in the life span characterized by: identity exploration, instability, self-focus,
feeling in-between adolescence and adulthood and feeling hopeful about future
possibilities (Arnett, 2013). More importantly, emerging adults do not exist in all
cultures and only exist in cultures (middle income) that allow the putting off of adult
roles and responsibilities (Arnett, 2013).
Recent national behavioral trends in transitioning into adulthood have shown
delays in traditional major life events such as age at marriage and parenthood,
instability of residence, higher rates of enrollment in college education and a decline
in emerging adults working for pay (Ingels, Glennie & Lauff, 2012; Arnett, 2013).
Arnett (2000 & 2013) characterizes the self-views of emerging adults, in addition to
not perceiving themselves as an adolescent or an adult, as also not fully accepting
responsibility and not making independent decisions. This may be especially difficult
for those who were born prematurely. In addition during the transition from
adolescence (ages 10-18) into emerging adulthood (ages 18-25) extensive related
endocrine system changes occur and influence bodily processes (Arnett, 2013). This
turbulence in endocrine hormones, involving all brain structures, adds to the life
experiences influencing brain growth and emotional health. An emerging adult born
premature may not have the flexibility or adaptability of the HPA axis responses to
achieve allostasis and resiliency.
Globally emerging adults are experiencing life as less meaningful and health
professionals are increasingly concerned about emerging adults negative behavioral
choices to deal with stress as a way of coping (Hutchinson, Stuart & Pretorius, 2007).
American adolescents and emerging adults have a higher rate of risk behaviors than
other countries (Arnett, 2013). Additionally, emerging adult college students were
more likely than older students to become angry or hostile about negative life events
instead of becoming more anxious and depressed (Jackson & Finney, 2002).
Emerging adults born premature who may have physical difficulties, learning
problems and limitations in social skills have an additional level of coping complexity
during this developmental period (Sullivan, 2008). Considering these challenges at
age 23, it may be expected that prematurely born emerging adults will have difficulty
coping with adult stressors.
During emerging adulthood, exploration and changes occur that often lead to
lasting life choices (Arnett, 2000) with stressors, coping styles and neurophysiological
responses of these life choices effecting overall health (Lovallo, 2005; Somerfield &
McCrae, 2000). Differences in stress exposure, appraisals of stress and coping styles
have been identified in adults with immune system disorders, cardiovascular,
depression disorders, and include a variety of physical and mental diseases (Cohen et
al, 2007; McEwen, Gray & Nasca, 2015; Segerstrom & Miller, 2004). Anxious
adults with comorbid depression have been found to use more emotion oriented
coping than individuals without a comorbid diagnosis (Man, Dugan, & Rector, 2012).
The role of avoidance coping has been associated with the generation of stress that a
decade later leads to depressive symptoms (Holahan, Moos, Holahan, Brennan &
Schutte, 2005).
Given that higher percentages of psychological problems were found at the age 17
original study time point of both gestationally small and premature infants and that
growth of the brain was not fully completed, then obtaining stress, coping, emotional
intelligence and emotional health measurements by examining the age 23 cohort will
provide additional developmental data.
Stress and Coping
Multiple definitions of stress and stressors exist and are often criticized as being
“circular, formless or varied (Aldwin, 2009)”. Indeed, stress is defined according to
each multiple discipline perspectives and applied to divergent topics (Aldwin, 2009).
Stress definitions have also been classified as: a response (Styles: physiological), a
stimulus (Holmes & Rahe: adaption to life events), a transaction (Lazarus &
Folkman: appraisals and coping), a dynamic process, state-like or trait-like and
acute or chronic (Rice, 2012; Lyons 2012; Butler, 1993).
Acute and chronic psychological stress in this study are defined by the DOHaD
theory. Acute stress is characterized by the ‘fight or flight” response and is short term
with transient over arousal, gastrointestinal symptoms, muscular problems and
combinations of the three stress emotions of anger or irritability, anxiety or depression
(Miller & Smith, 2015). The American Psychological Association (2015) also
defines an “episodic acute stress” characterized by an “individual always in chaos, in
a hurry, full of nervous energy and type A personalities.” Chronic stress, is the daily
wear and tear of allostatic load and can lead to “suicide, violence, heart attack, and
stoke (Miller & Smith, 2015)”.
Related to types of stress are the Diagnostic and Statistical Manual of Mental
Disorders, 5th Edition (DSM-5; APA, 2013) broad definition of anxiety disorders.
Anxiety disorders have “features of excessive fears, anxiety and related behavioral
disturbances (p 189)”. “Fear is the emotional response to real or perceived
imminent threat, resulting in arousal of the flight or fight response, and anxiety is the
anticipation of the future (p 189),(APA, 2013).”
Measuring stressors is often done by checklists and interviews (Gutman &
Nemeroff, 2011). A number of functional tests of HPA activity have been developed
including the dexamethasone (DST) suppression test, the corticotrophin-releasing
factor (CRF) stimulation test and the combined (DEX/CRF) test. These tests are
invasively administered or use oral administration (Gutman & Nemeroff, 2011). The
Trier Social Stress Test (TSST) a reliable non-invasive psychological challenge test
was developed to test HPA axis reactivity to psychological stressors (Gutman &
Nemeroff, 2011). A standardized laboratory protocol involves a 10-minute public
speech and a mental arithmetic test. The TSST combines both uncontrollability and
evaluative threat, which are the conditions of DOHaD theory to activate the HPA axis
response (Kudiela, 2008). As a result the response to TSST is both physiological and
psychological including increased anxiety and negative mood (Kirschbaum, 2010).
TSST testing has shown that total plasma cortisol levels are overall higher in
elderly women when compared to elderly men (mean age 67.3 years), younger men
and women (mean age 23.5 years) and without any differences in the patterns of
reactivity (Kudielka, Buske-Kirschbaum, Hellhammer & Kirschbaum, 2004).
Schommer, et al., (2003) found habituation to psychosocial stressors unchanged
overtime even if an individual was found to be a “high” or “low” cortisol responder to
the TSST. Meaning, that the cortisol response to stress pattern remains uniform when
activated with repeated stress. Additionally differences in cortisol response to TSST
have been found in many psychological disorders (McGirr, Daiaconu, Berlim,
Pruessner, Sable, Cabot & Turecki, 2010).
Maltreated female youths (ages 12-16 year) show a different cortisol pattern in
response to the TSST (McMillan, et al., 2009). Youth without a history of
maltreatment showed an increase of cortisol followed by a gradual decline, in contrast
to youths with a history of maltreatment, who showed no increase in cortisol in
response to the TSST and no decline. Emerging adults, at age 23, who were born
preterm are expected to have a pattern of salivary cortisol response of little to no
increase and little to no decline after exposure to the TSST. Total cortisol levels may
vary in comparison to the full term born by being higher.
Lazarus and Folkman’s enduring model (Carver, 2011) of psychological stress
and coping responses focuses on the process between the person, environment, their
appraisal of and context of the event and is consistent with DOHaD theory (Lazarus,
1999; Park & Folkman, 1997). Psychological stress is what happens when a person
is defeated in obtaining their goal commitment, intention or values (Lazarus, 1999).
Stress mediating processes include coping responses defined as problem and emotion
focused resulting from the primary and/or secondary appraisals used and are
considered psychologically effective if they work for the individual (Lazarus, 1999).
Moos and Holahan, (2003), added dispositional (inclined to cope) factors resulting
in two orientations: focus and method of coping. The focus is either approach or
avoidance while the methods of coping are cognitive and behavioral (Billings &
Moos, 1981; Moos, 1995; Moos & Holahan, 2003). Approach coping is defined as
problem solving attempts to deal with and resolve stressors while avoidance coping
is defined as emotion focused attempts to avoid dealing with, thinking about, and
managing emotions associated with the stressor (Moos & Holahan, 2003).
Combining the focus and methods of coping results in eight coping subset styles listed
in Table 1 and defined in Table 2, and are measurable with standardized self-report
instruments.
Moos and Holahan’s definition of coping is one of three models (Aldwin, 2009;
Rice, 2012). Two of the three other models explaining coping are: the environmental
system, addressing ongoing life stressor and social resources, and the personal system
involving individual demographics (Rice, 2012). The third model, transactional,
incorporates personal and contextual factors of the stress situation with coping skills
that affects the psychosocial functioning and maturation at the individual’s next stage
of development (Rice, 2012). Determinants of coping responses are the types and the
severity of the stress, social resources and demographics (Rice, 2012). Gender, age,
education, SES, cognitive abilities, problem-solving skills and personal control or
regulation will effect both the focus and method of coping.
Table 1
Coping Styles
Type of Coping Approach Coping Avoidance Coping
_____________________________________________________________________________________________
Cognitive Logical Analysis Cognitive Avoidance
Positive Reappraisal Acceptance/Resignation
_____________________________________________________________________________________________
Behavioral Seeking Guidance and Support Seeking Alternative Rewards
Problem Solving Emotion Discharge
____________________________________________________________________________________________
Table 1. From “Dispositional and Contextual Perspectives on Coping: Toward an Integrative Framework,” by R. H. Moos and C. J. Holahan, 2003, Journal of Clinical
Psychology, 59 (12), p.1391. Copyright 2003 Wiley Periodicals, Inc. Adapted with permission.
Table 2
Definitions of Coping Styles (Moos & Holahan, 2003)
___________________________________________________________________
COGNITIVE APPROACH COPING Combination of logical analysis and
positive appraisal strategies
Logical Analysis Attention to one aspect of the situation
Utilizing past experiences
Thinking about possible actions and their
consequences
Positive Appraisal Accepting situation and restructuring it in
a favorable way
_____________________________________________________________________
BEHAVIORAL APPROACH COPING Dealing directly with situation through
concrete actions
Seeking Guidance and Support Seeking guidance and support from others
Problem Solving Actions derived from the approach
strategy, and organized information about
the problem along with the allocation of
resources, monitoring progress and
evaluating results (Cherry, 2013)
COGNITIVE AVOIDANCE COPING Combination of cognitive avoidance and
acceptance or resignation.
Cognitive Avoidance Minimizing or denying the situation and/or
consequences
Acceptance/Resignation Accepting the situation and/or
consequences and deciding it cannot be
altered.
____________________________________________________________________
BEHAVIORAL AVOIDANCE Involves seeking alternative rewards,
venting feelings and/or engaging in risky
behaviors.
Seeking Alternative Rewards Replacing loses with involvement in new
activities resulting in an alternative source
of satisfaction
Emotional Discharge Openly venting feelings of anger and
frustration
Behaviors that temporarily reduce tension
involving acting impulsively and/or doing
something risky
_____________________________________________________________________
Table 2. From “Dispositional and Contextual Perspectives on Coping: Toward an Integrative Framework,” by R. H. Moos and C. J. Holahan, 2003, Journal of Clinical
Psychology, 59(12), p.1391. Copyright 2003 Wiley Periodicals, Inc. Adapted with permission.
Gender Differences in Stress and Coping
The American Psychological Association (APA, 2010) reports differences in the
way males and females react to, manage, and view their ability to deal with stress. In
general: females report more stress than males (especially married females), more
physical symptoms of stress, and identify money and economy more often as sources
of stress while males report work more often as a source (APA, 2010).
Matud (2004) examined stress and coping differences between genders and found
outcomes consistent with decades of past research. There were no significant
differences in life event frequencies experienced between genders, yet females
reported life events as more negative (p = <0.05), less controllable (p =<0.01) and
also reported more chronic stress (p = <0.01) than males. The major stressors for
females were family and health related while males’ stressors were focused on
relationships, finances and work events. Females utilized emotional and avoidance
coping styles more frequently while males used less emotional coping (p < 0.001).
Females experienced more psychological distress (p < 0.001) and somatic symptoms
(p = <0.001) than males.
Tamres, Janicki and Helgeson (2002) in their meta-analysis of gender coping
differences reviewed 50 English language empirical studies between the years of
1990-2000, with actual stressor measurements rather than hypothetical situations, to
examine coping responses. The authors categorized the studies’ definitions of
coping behaviors into problem-focused and emotional-focused with avoidance,
approach-based and other components. Females showed a wider repertoire of types
of coping behaviors with higher usage of most types than males. Significantly,
females used more verbal, social support seeking, ruminating and positive self -talk
than males. A few differences between genders were found with females more often
than males using avoidance responses for coping with other’s health stressors while
males used avoidance responses for coping with relationship stressors.
Gender differences in coping patterns at emerging adulthood (ages 18-25 years)
have been found to reflect established cultural qualities (Davis, Burleson &
Krusewski, 2011; Kim & Sasaki, 2014) with endorsement of masculinity as a
significant predictor in problem-oriented coping (Lipinska-Grobelny, 2011). A
recent decline in female gender depressive symptoms in emerging adults is thought to
be associated with greater autonomy and empowerment (Frye & Liem, 2011) although
in general, females had been found to have higher emotional coping than men (Durm
& Glaze, 2002).
DOHaD, Stress and Coping
DOHaD theory focuses on the HPA Axis physiological and biochemical
mechanisms and how these interact, as well as, the resultant effects on higher nervous
system processes such as behaviors, cognitions and emotions. Importantly, DOHaD
theory defines stress as a real or perceived threat (physical or psychological), a
stressor as an aversive stimuli and the stress response as the activation of numerous
complex body systems through the HPA axis. Accordingly, stress, coping responses
and affective states are thought to influence physical pathology by direct and indirect
Figure 6
Relationship of Hippocampus to HPA Axis
Figure 6. Reprinted by permission from Macmillan Publishers, Ltd: Nature Neuroscience, “How Adversity Gets Under the Skin” by Steven E Hyman,2009, Nature Neuroscience, 12, 241-243. Copyright 2009 by Macmillan Publishers, Ltd.
influences on the biological processes and behavioral responses with the HPA Axis
seen as the gateway (Cohen, Janiki-Deverts & Miller, 2007; Heindel & Vandenberg,
2015; Lovallo, 2005; Somerfield & McCrea, 2000). The roles of allostasis and
allostatic load above all, is the link provided as a mediator of the accommodation to
the stressor, being that system-wide physiological changes are made and the HPA
Axis interconnects with other brain areas including the prefrontal cortex (PFC) to fit or
adapt to the situation (McEwen, Nasca & Gray, 2015; McEwen, 1998, Ganzel, Morris
& Werthington, 2010), (See Figure 6). Figure 5 illustrates “the HPA axis under the
excitatory control of the amygdala and inhibitory control of the hippocampus (Hyman,
2009)”.
Importantly, studies of individuals experienced in meditation, show related
inverse changes in functional brain imagery and mapping of brain activity (Hoffman,
et al., 1982). When relaxation increases, heart rate, blood pressure and hippocampus
signal activity decreases (Hoffman et al.,1982). Individuals with years of meditation
experience also show thickening of the frontal cortex of the brain (Lazar, et al., 2005).
The researchers think genomic charges are taking place from meditation relaxation
since, in addition to sympathetic nervous system responses, chemical changes related
to gene changes had been identified. The gene changes are believed to be a
counterpart of the stress reduction response (Dusek, et al., 2008).
The resultant system-wide and HPA-Axis responses to stress (appraisal of threat)
and the stressor (aversive stimuli) allows for the inclusion of appraisal, cognition and
emotional states as key elements of the stress process. Hence, DOHaD theory
advances an integrated model of stress through multilevel biomedical and
psychosocial models of stress (Ganzel, Morris, & Wethington, 2011). Inherent in
dealing with stress are the efforts to manage the potential and threatening aspects of
the situation or circumstances, whether physical or psychological, and any detrimental
consequences to health (Moradi, Pishva, Ehsan, Hadadi, & Pouladi, 2011).
Psychologically, coping is defined as changing cognitively and behaviorally to mange
internal or external demands that extend beyond the persons existing resources
(Lazarus & Folkman, 1984).
Emotional Intelligence
A variety of emotional intelligence definitions were found in a systematic
literature review, using the keywords “emotional intelligence”, from the Cumulative
Index of Nursing and Allied Health Literature (CINAHL), Cochrane Library,
ProQuest Dissertations, PubMed and the Web of Science. The majority of
publications were from the disciplines of psychology and business with proliferation
of the topic in psychology beginning in the early 2000’s (Matthews, Zeider & Roberts,
2004). Recently, the nursing literature on EI has shown an interest in the
epistemology, application to educational and the professional competences uses of the
construct (Por, Barriball, Fitzpatrick & Roberts, 2011; Akerjordet & Severinsson,
2010; Smith, Profette-McGrath & Cummings, 2009; Freshwater & Stickley, 2004;
McQueen, 2004). A large body of literature exists in the business arena where EI is
extensively used in hiring, employee assessments, promotions and education of
managers (Ashkanasy, Ashton-James, & Jordan, 2004; Freedman, 2010).
One aspect of EI in which all agree is the involvement of an emotional awareness
of self and others and emotional regulation or management (Armstrong, Galligan, &
Critchly, 2011; Matthews, Zeider & Roberts, 2007 & 2004; Bar-On & Parker, 2000).
A broad common definition of EI is the capacity to identify, process and manage
emotions to contribute to a successful life (Armstrong, Galligan, & Critchly, 2011).
Emotional regulation is used interchangeably with emotional management and is
defined as the conscious or unconscious control of emotion, mood, and affect that is
most commonly achieved through coping strategies (Kowalczyk, 2015; Thompson,
1994). The construct of EI developed out of the research on intelligence to bridge a
gap in the role of emotions and is widely used today in education and business settings
(Mayer, Salovey, & Caruso, 2004).
Multiple studies have indicated a relationship between stress, coping styles, EI
and emotional health (Por, Barriball, Fitzpatrick & Roberts, 2011; Tricky, Far hall,
Wertheim, Hinch & Ong, 2011; Ciarrochi, et al., 2002; Gerits, Derkson, Verbruggen
& Katzo, 2005). Studies have found that individuals with high EI report less
perceived stress, have better health and report feelings of well being (Ciarrochi, et al.,
2002; Hertel, Schutz & Lammers, 2009; Pau and Croucher, 2003). Individuals with
low EI reported more stress and difficulties with coping (Gohm 2005; Schutte,
Malouff, Thorsteinsson, Bhullar, & Rooke, 2007). Cirrochi, Deane & Anderson,
2000, found stress associated with higher reports of depression, hopelessness, and
suicide ideation in college students (N = 302) with high emotional perception scores
and found more suicide ideation in college students who scored low in managing
others emotions.
The reciprocal relationships between stress, coping and the hippocampus and how
it relates to emotional intelligence warrants further investigation as recent studies are
finding smaller hippocampal volumes in individuals with long-term Post Traumatic
Stress Disorders (PTSD), (Woodward, et l., 2006), (See Figure 6). Impairment has
been found in fear responses of individuals with PTSD involving dysfunctional
activation of the HPA Axis and especially within the ventromedial prefrontal cortex
(Milad et al., 2009). EI can predict health functioning as well as distress and
traumatic stress (Singh & Sharma, 2012). Additionally, oxidation of cells occurs
from psychosocial stress and reflects an increase in cell aging (Fricchione, 2015).
Singh and Sharma (2012) also found high levels of salivary cortisol improve coping
strategies in individuals with high EI while Tang, et al., (2007) found a significant
decrease in stress-related cortisol with 5 days of 20-minute meditation improving
attention and self-regulation.
Infants born prematurely have a variety of health impairments and a prevalence of
neurodevelopmental disabilities in general (Allen, Cristoalo & Kim, 2011). Attention
issues and ineffective executive functioning has been found in premature low birth
weight infants suggesting that regulation of these functions in the cerebral cortex may
have been impaired (Kessenich, 2003). This area of the brain is also utilized in
regulating emotions, interpreting and organizing information for responses which
influences the level of an individuals’ EI (Contrada & Baum, 2011). Premature
emerging adults who may have perinatal injury and experienced sensitive time periods
of stress effecting the HPA Axis, then are exposed to increasing vulnerabilities to
stress, coping, and allostatic load during this time period, may have responses that
negatively effect EI (Allen, Cristofalo & Kim 2011; Hack, 2009; Ozer &
Benet-Martinez, 2006). EI studies of emerging adults, ages 18-25 years old, are
scarce and the majority of studies are cross-sectional with mixed adult age ranges of
the participants. Current measurement of the abilities to lead a successful life often
are functional and relate to developmental milestones determined by age-appropriate
roles, succeeding in schoolwork, succeeding in the work environment, social
maneuverability and forming intimate relationships to mention a few (Sullivan, Msall,
& Miller, 2012). Given the identified vulnerabilities of prematurely born infants then
measuring and describing EI in this population at age 23, including gender differences,
may lead to further understanding of possible predictive functions, critical time
periods of risk, protective factors and types of effective clinical interventions. “What
is not known is what are the long-term outcomes for adults who were born
prematurely and how does stress, biology, caregiving and social factors over a
lifetime effect the developing premature born infant? (Sullivan, 2008-2013)”.
EI Theoretical Perspectives
Historically, the modern origins of EI can be traced back to John Dewey (1902)
“moral motive” and then Thorndike’s 1902 conceptualization of “social intelligence”,
which at a rudimentary level, involves the ability to understand and mange other
people while getting along socially (Cantor, 2000; Zeidner, Matthews & Roberts,
2009). Social intelligence was later eclipsed by interest in EI that included
differentiating between cognitive, emotional and other factors. EI began to capture
scientific interest in academic journals during the early 1990’s through publications by
Mayer and Salovey’s model as a way of joining emotions to intelligence studies
(Mayer, Salovey & Caruso, 2000). Culturally, Goleman popularized EI in the 1995
publication of the book Emotional Intelligence that integrated emotions with
intelligence. The importance of both emotion and reason intuitively appealed to the
public and some in the scientific community (Matthews, Zeider and Roberts, 2004).
Although the scientific community is studying EI there is not agreement on whether it
is a scientific endeavor or if there is a science of EI (Zeidner, Matthews & Roberts,
2009). A discussion of the theories, measurements, and applications of EI to this
controversy follow.
The term EI is used in three ways (Mayer, Salvey, & Carusi, 2000): 1. The
popular meaning is that reason and emotion can be personally integrated and an
individual can achieve self-improvement. 2. To describe personality traits through
connecting parts of the mind to life outcomes from mental mechanisms, models of
self, and self-relevant and general traits. 3. To define a set of abilities dealing with
processing emotional information. Three theorists have influenced the development
of EI knowledge, the use in practice, and research across multiple disciplines: Daniel
Goleman, Mayer & Salovey, and Raven Bar-On (Smith, Profetto-McGrath &
Cummings, 2009).
Goleman’s theories developed from the business sector and popularized the
concept of EI through use of work competency measures that covered a broad range of
personality measures (Mayer, Salovey & Caruso, 2004). EI to Goleman consist of
five parts: “ knowing emotions, managing emotions, motivating oneself, recognizing
emotions in others, and handling relationships, (Goldman, Boyatzis and Hay Group,
2005).” The five parts have been divided into 25 different competencies and include
mapping of these competencies. Goleman’s model is a combination of theoretical
concepts and construct derived from multiple psychological perspectives resulting in a
popular, trait and ability mixed model. The model has wide spread popular appeal
and is viewed as over inclusive by some in the scientific community. Goleman,
Boyatzis and Hay Group (2005) developed the self-report, Emotional and Social
Competency Inventory (ESCI), to assess the emotional and social competencies of
outstanding leaders and provided guideline for using the ESCI. Courses and
certifications in EI are also available. Extensive construct and validity studies within
business organizations worldwide have been conducted. Overall, reliability has
shown high internal consistency with limited evidence for test-retest reliability. EI
has good construct validity with a variety of personality constructs (Wolf, 2005).
Mayer, Salovey & Carusso, 2000, ability model views EI as operating across both
cognition and emotional systems as a “unitary intelligence “ (Mayer, Salovey &
Carusso, 2000; DeFabio & Saklofske, 2014). Emphasis is on EI as a “concept of an
intelligence that processes and benefits from emotion” and is composed of “mental
abilities, skills or capacities”. The unifying system has 4 branches: emotional
perception (perceive, attend, decipher and express), emotional integration (uses
cognitive system), emotional understanding (understanding and reasoning) and
emotional management (flexible guidelines to mange emotions). EI is conceptualized
as a mental ability and measured with objective tasks. The Mayer-Salovey-Caruso
Emotional Intelligence Test (MSCIET) measures EI by having the individual perform
tasks and solve emotional problems in 4 areas: perceiving emotions, facilitating
thought, understanding emotions and managing emotions (Mayer, Salovery & Caruso,
2004b). The original measurement had criticisms relating to scoring and reliability
and a second version addressing some of these issues are now in use (Mayer, Salovey,
Caruso & Sitrenious, 2001).
Bar-On, 1997, generally classified as a trait model and by some others as a
mixed model defines EI as an “array of non-cognitive capacities, competences and
skills that influence one’s ability to succeed in coping with environmental demands
and pressures” (Bar-On, 1997; DiFabio & Saklofse,2014; Por, Barriball, Fitzpatrick
& Roberts, 2011). Bar-On and Parker (2000) view the key elements of EI as stress
management and the ability to adapt. The self-report trait EI, in this study, was
assessed with the Bar-On EQ-I. The 133 likert-like item questionnaire provides a
total EI score (M = 100, SD = 15), and five composite scores for the principle
dimensions with 15 related content scale scores (Bar-On, 2002 & 2006; Di Fabio &
Saklofske, 2014; De Weerdt & Rossi, 2012). The five composite score areas are:
intrapersonal, interpersonal, adaptability, stress management and happiness (Bar-On,
2002 & 2006; Di Fabio & Saklofske, 2014; De Weerdt & Rossi, 2012). The 15
content scale scores are: emotional self-awareness, assertiveness, self-regard,
self-actualization, independence, empathy, interpersonal relationship, social
responsibility, problem solving, reality testing, flexibility, stress tolerance, impulse
control, happiness and optimism (Bar-On, 2002 & 2006; Di Fabio & Saklofske, 2014;
De Weerdt & Rossi, 2012). The model evolved from personality psychology and is
measured through a standardized self-report test that assessesself-perceptions rather
than actual abilities (Mayer, Salovey, & Carusso, 2000). Studies show the EQi has a
significantly stronger association with mental health than other measures (Gohm
2005; Schutte, Malouff, Thorsteinsson, Bhullar, & Rooke, 2007). Raven Bar-On
EQi test is used in this study to assess EI, stress management, adaptability and general
mood.
A major issue and controversy with EI definitions is they vary so determining
what processes, behaviors and outcomes are related makes operationalization of the
construct difficult if not possible and limits hypothesis testing (Bar-On & Parker,
2000). A construct is deliberately and consciously invented or adapted for a specific
purpose and identifies what meets inclusion or exclusion by categorization (Mishra,
2013; WSU, 2013). In addition, constructs serve as an indirect link between the
abstraction defined and observed manifestations, in contrast to concepts which are
directly linked with observation (WSU, 2013). Construct validity includes assessing
the test content, response processes, internal structure, association with other variables
and consequences of its use (Furr & Bacharach, 2014). Construct validity in EI is, at
best questionable, as definitions of EI measurements are based on multiple theories
and not on an accurate and agreed upon representation of the entire domain (Stough,
Saklofske, & Parker, 2009). As with many constructs in the social sciences, face
validity and content validity refers to the scores derived from each test item and not
the test, and is often also an issue with other social science constructs (Stough,
Saklofske, & Parker, 2009). Conceptualization of EI on face validity is appealing yet
construct validity across measurements has not been achieved. Research has shown
that ability based and self-reported trait EI tests are not correlated yet differing models
of trait self-reported EI were found to be correlated despite describing similar and not
identical constructs (DiFaboe & Saklofske, 2015). EI developed from personality
theories and maybe redundant with personality constructs (Stough, Saklofske &
Parker, 2009).
DiFabeo & Saklofske, 2014, administered a battery of eight tests to assess
emotional intelligence (including Raven Bar-On), self-evaluating, resilience, and life
satisfaction, to 164 Italian high school students, and utilized multiple regression for
the data analysis. Significant results were found for the ‘Big 5” personality factors
followed by trait self-reported emotional intelligence tests as the most predictive of
self-evaluation, resilience and life satisfaction. An equally significant finding, was
the higher the self-reported trait EI score then the more positive, in control, able to
deal with adversity and emotional resources available were perceived by the
individual.
Summary
In summary, the construct of EI, is primarily based on personality theories, and
measurements lack construct validity across tests. On the other hand, EI theories are
used in business, educational and health settings, and are capturing components or
factors related to success in dealing with stress, coping, emotional management and
getting along with others socially. The Bar-On EQi, captures emotional and
psychological functioning, fits with DOHaD theory, and was utilized in this study to
assess the emotional development of emerging adults and any differences between the
prematurely and full term born. Although definitions of EI vary and a unified
construct validity has not been achieved, EI is in wide use, and the appeal may be the
ability to capture assessments of traits of a mature personality as demonstrated in the
study above conducted by DiFabeo & Saklofske (2014). Additionally, emotional
intelligence scores level off and usually without further gain in adulthood, and this
could be related to personality development theories (Garner, Qualter, & Whitely,
2011). Thus, the measurement of EI at early or emerging adulthood is very relevant.
The Daily Hassles Questionnaire will provide a standardized measure of usual
life stress events. Moos & Billings (1981) determinates of coping styles provides the
coping types and strategies used by an individual in stressful events, and carried over
from any previous stressful experiences while fitting conceptually with EI (Moradi,
Pishva, Ehsan, et al., 2011. Bar-On and Parker (2000) view the key elements of EI as
stress management and the ability to adapt. Elements from each of these
perspectives, a long with coping strategies and stress responses have been implicated
in health issues.
Emotional Health
Health, well-being, mental health and quality of life are similar concepts, which
include biology and the individual’s psychological state, to utilize goal directed
behaviors and involve multiple causal networks (CDC, 2013). Emotional health is
defined as an individual “adjusting to new situations and achieving the desired
outcomes” (GUCCHD, 2016). Higher emotional intelligence maybe related to better
emotional health and is linked to aspects of better psychosocial functioning (Schutte,
Malouff, Thorsteinnsson, Bhuller & Rooke, 2007). Drug use, being bullied and
violence are a few of the behavioral risk factors that threaten emerging adults
emotional health globally (Lister, Merrill, Vance, West, Hall & Crookston, 2015;
Orleans, 2008). There is a range of emotional behavior dependent on an individual’s
adaptation to stress and coping style, resulting in effects on feelings of well-being,
functioning and health behaviors (Glanz & Schwartz, 2008).
Childhood physical and emotional abuse is related to childhood psychiatric
disorders and also effects cortisol (HPA) stress reactivity (MacMillan, Tanka, Duku,
Vaillancourt & Boyle, 2013; MacMillan, et al., 2009). Children and adolescents
mental health, according to the CDC (Perou, et al., 2013) is characterized by meeting
developmental and emotional milestones, social development, effective coping skills,
and being able to function at home, school and other areas of their life. A similar
definition of emotional health exists for emerging adults (Arnett, 2013). A number of
studies of emerging adults show their identified markers of transition are: “accepting
responsibilities for oneself, making independent decisions and becoming financially
independent (Arnett, 2013; Nelson, 2003).” Additionally, social and emotional
loneliness is common and often used for self-reflection and mood management
(Arnett, 2013). High EI scores were associated social functioning, mental health, and
vitality (Rey & Extremera, 2013). EI has been found to have a moderate positive
relationship with coping styles and buffered stress in work situations (Gujral, 2013).
Health experts have agreed that most physical problems begin in the early teens
through the early 20’s and relate this to behavior patterns developed during this time
period (Arnett, 2013). As a result, these patterns of behavior, become established
and effect adulthood responses. Health educational programs, directed at risky
behaviors have shown mixed results (Arnett, 2013). Effective psychosocial
protective factors have been identified, such as exercise that improves mood, weakens
the stress response and is thought to promote neurogenesis, while reinterpreting
negative stress stimuli through cognitive positive reframing involves memory, control
of emotion, and underlying neurobiology (Feder, Nestler & Charney, 2009).
Tsaousis & Nikolaou, 2005, through two studies (N = 365 & N = 212) with mean
age ranges of 25-36 years old measured: 1. EI and general health in one group and
2. EI, general health and health related behaviors (smoking, drinking, and exercise) in
another group. EI was found to be negatively associated with poor general health,
negatively correlated with smoking and drinking and positively correlated with
exercise.
Burnett, et al., in 2011, conducted a meta-analysis of peer-reviewed research
article findings from 1995-2010. The purpose was to look at “the prevalence of
psychiatric diagnoses in preterm and full-term children, adolescent and young adults.
(Burnett, 2011).” Of 719 articles only 5 passed inclusion and exclusion criteria
resulting in 734 preterm and 634 full term (controls) individuals. The study reported
high odds ratio of risk for anxiety, depression and other psychiatric disorders in the
prematurely born.
England’s young adults (between the ages of 18 and 25 years old) were found to
have resilience-related coping skills by utilizing social support when compared to
older adults (ages > 64 years old) who were more resilient and utilized emotional
regulation and problem solving (Gooding, Hurst, Johnson & Tarrier, 2011). EI
research has shown an association with better health and is a plausible health predictor
(Martins, Ramalho & Morin, 2010; Schutte, et al., 2007).
Adolescents with visible or invisible chronic health conditions (disabilities) were
found to do less well in several psychological study outcomes than adolescents
without disabilities (Wolman, Resnick, Harris, & Blum, 1994). One similar invisible
condition is Alexithymia, broadly defined “as an inability to express one’s feelings
(Merriam-Webster Medical Dictionary, 2015)”. Some researcher postulate this
condition is due to deficits in cognitive processing of emotions resulting in
undifferentiated poorly regulated emotions and representative of the opposite of
emotional intelligence (Velasco, Fernandez, Paez & Campos, 2006; Taylor, Bagby &
Parker, 1991). Recent research developments have associated alexithymia with
maladaptive emotional regulation, low EI, reduced rapid eye movements, somatic
illness, and disease development (Taylor, 2000; Taylor, Bagby & Parker, 1991).
Given the potential for disabilities due to HPA axis, emotional dysregulation in
emerging adults born prematurely, coupled with previously mentioned higher
incidences of psychiatric disorders, then a range of developmental functioning,
well-being and psychopathologies are possible. Indeed, if self-emotional regulation is
a part of EI, then the prematurely born are at risk for self-regulation and mental health
disorders especially Attention Deficit Hyperactive Disorder (ADHD), (Sullivan,
personal communication, November 11, 2014).
Summary
In this study measures for assessing stress responses, coping types, emotional
intelligence and emotional health are utilized. The TSST provided physiological
responses by inducing a moderate stress situation along with salivary cortisol levels to
assess HPA regulation. The DHS provided self-reports of everyday stress experiences
as representative of developmental milestones as well as stress magnitude scores in all
perinatal birth groups. The Bar-On EQi (1997), total EQi score indicates the
emotional intelligence levels in the perinatal birth groups. The ASR provides a
emotional health score for all participants. Comparisons of emotional health and
stress reactivity of salivary cortisol levels determine if any differences between
perinatal birth groups exist.
HPA Axis and the Stress Response
The stress response consists of activation of two brain pathways triggered by the
hypothalamus. The first pathway involves the autonomous nervous system and
release of epinephrine causing the physiological response of fight or flight. This
pathway’s response is described by Selye’s theory of adaptation to stress definition of
immediate responses (Arnold & Kverno, 2009).
The second pathway involved in the stress response is the anterior HPA Axis.
Stress, directly and indirectly affects the HPA Axis, initiating the stress hormonal
response at the hippocampus level (Figure 7). The primary hormone regulating this
axis is the glucocorticoid, cortisol (Edmunds & Mayhew, 2009).
The HPA Axis, consisting of the hypothalamus, pituitary and adrenal gland,
regulates cortisol secretion from the adrenal glands whenever we are stressed and
produces a physiological response (Bruyere, 2009). Corticotrophin-releasing
hormone (CRH) from the hypothalamus acts as a chemical messenger to the pituitary
gland. In turn the pituitary gland responds to the CRH and releases
adrenocorticotropic hormone (ACTH) into the blood stream. The circulating ACTH
in the bloodstream reaches the adrenal gland that then produces and releases
cortisol. The cortisol circulates in the bloodstream until the demand for it is met.
Physiologically, there is a cascade of effects including increased cardiac output, pupil
dilation, and shunting of blood from the digestive tract and kidneys to vital organs
ultimately resulting in decreased fluid loss, increased glucose, and decreased brain
nor-epinephrine. Once the demand is satisfied the cortisol signals the pituitary to
stop producing ACTH.
Figure 7
Corticotropin Releasing Factor System
Figure 7. Reprinted with permission by Sage College. In W. Lovallo, (2005), Stress and health: Biological and psychological interactions (p 116). USA: Sage Publications. Copyright 2005 by Sage College.
The production of cortisol in the HPA axis is regulated through a negative feedback
loop system:
adrenocorticotropic hormone or acetylcholine (ACTH).
decrease of cortisol production (Edmunds & Mayhew, 2009).
When the HPA Axis is functioning effectively the endocrine response will be
quick and adaptive. If the HPA Axis is exposed to abnormal allostatic loads, defined
as repeated stress, lack of an adaptive response, or an inadequate response then
dysregulation occurs or allostasis is not achieved, resulting in variations in the cortisol
levels (Barker, 1990 & 2007).
Cortisol is the end product of the HPA Axis chemical transactions (de Weerth,
Zijl & Buitelaar, 2003). Cortisol levels follow a circadian or diurnal pattern in normal
adults totaling a secretion level of 10 mg. a day (Edmund & Mayhew, 2009). Cortisol
levels are highest in the early morning, peak 60 to 90 minutes after awakening, and are
lowest from evening to midnight (Edmund & Mayhew, 2009).
The processes involved in the HPA Axis negative feedback loop are complex and
influenced by a number of multifaceted variables. The timing of sampling during
this process of cortisol circulation will affect the interpretation of results nonetheless
standardized timeline comparisons and interpretations are available for adults and
children (de Weerth, Zijl & Buitelaar, 2003).
The cortisol feedback loop, also involves circulation to the frontal cortex and
limbic areas, which effects affective responses and past experiences (Lovallo, 2005).
Differences in the frontal-limbic system as part of the central cortisol feedback system
will in turn influence the differences in the stress response (Lovallo, 2005).
Summary
In summary, cortisol is a key stress response glucocorticoid within the HPA Axis
and prefrontal cortex negative feedback loop response. Cortisol can be accurately
measured in the saliva as well as the blood, and patterns of responses are standardized.
Changes in HPA Axis responses may help identify periods of transition into disease
states. Salivary cortisol, in this study, was measured to obtain the HPA stress
response pattern in a sample of former premature infants and a term born comparison
group at age 23 years. The cortisol response was examined in association with
self-reported stress and coping patterns, as well as emotional intelligence and
emotional health.
HPA Axis Function in Prematurity
Prematurity rates in the United States contribute to national health care issues and
costs both in the short and long term. The rate of premature birth for two and
one-half decades, from 1980-2006, increased by 20% (Martin, Osterman & Sutton,
2010). Twelve percent of all births in 2010, were premature, totaling 523,033 births
for the year (CDC, 2010). Currently the mortality rates for premature newborns with
low birth weights has decreased by around 2% due to newer preventative and
treatment approaches, but long-term morbidity remains (Child Trends Databank,
2011). This decrease in mortality rates has increased the rates of immediate preterm
birth consequences such as: adrenal insufficiency, intraventricular hemorrhage, patent
ductus arteriosus, respiratory distress syndrome, bronchopulmonary dysplasia,
necrotizing enterocolitis and retinopathy of prematurity (March of Dimes, 2008).
The long-term outcomes for these infants of decades of premature birth will
continue to influence social, educational, community, and family systems well into the
future. Prematurity in general has multiple immediate birth-related health issues,
and requires continued vigilance throughout childhood (Saigal & Doyle, 2008;
Sullivan, et al., 2008; Hack, Taylor, Drotar, Schluchter, Carter, Andreias, et al.,
2005; Saigal, Burrows, Stoskopf, Rosenbaum, & Streiner, 2000). More recently,
prematurity effects are proposed to contribute to the development of adulthood
illnesses (Hack, 2009; Saigal & Doyle, 2008).
In addition to the specific issues surrounding prematurity, the study of cortisol
levels as an indicator of the HPA Axis functioning in those born at term has
implications for application to health issues. Identifying any difference between
premature and full term birth HPA Axis functioning by screening for alterations in
cortisol levels in combination with stress, coping, emotional intelligence and
emotional health measurements may identify vulnerable individuals of all birth group
types before expression of any variations (Dedovic, Duchesne, Dager & Pruessner,
2010).
Cortisol levels in newborns have been hard to standardize due the rapid shifting of
development, instability of the newborn system and brain volume growth of
15mL/week between 29 and 41 week’s gestation (Main, 2010). No normal range of
preterm cortisol levels exist because of a variety of fluctuation in preterm and full term
physiological homeostasis (Ng, 2011). There is agreement that around 1 year of age
preterm cortisol levels begin to stabilize into a pattern approximating the adult diurnal
cycle (de Weerth, Zijl & Buitelaar, 2003). Under normal conditions, with full term
infants, cortisol levels reveal a circadian rhythm with the adult pattern of diurnal
decline from morning to evening at around 3 months of age (Turner-Cobb, 2005).
Attempts to collect salivary cortisol levels from newborns have met with issues of
lack of sufficient saliva quantity and concerns about interference of administered
sweet solutions (Morelius, Nelson & Theodorsson, 2004). Morelius, Nelson
& Theodorson (2004), successfully obtained 113 preterm and term infant’s saliva
using less than a 10mL sample. In combination with altering the detection limit of the
radio-immunoassay they were able to analyze very low concentrations of cortisol in
newborns without interference from oral glucose solutions.
Jansen, Beijers, Riksen & de Weerth (2010), analyzed 48 peer reviewed empirical
studies (1978-2008) providing pre and post stressor cortisol levels at various ages.
In the first 13 weeks or 3 months post-natal the mean cortisol reactivity effect to
painful stimuli was the highest and continued to decline with advancing infant age
groups (3 & 6 months, 6 & 12 months and 12 & 24 months).
Tollenaar, et al. (2010), obtained daily eye swab cortisol levels from 300 infants at
the ages of 6 weeks, 5 months and 12 months. The infant’s cortisol levels declined
over the year however intra-individual variability was large and stabilized between 5
to 8 months.
Knowing that the newborn’s system, whether preterm or full term, is continuing to
evolve at a rapid pace, understanding the processing of a variety of stressors during
critical growth periods become paramount. Prematurity is a stressor itself due to the
immaturity of the central nervous system and the neonatal course, which may include
neonatal illness and a long intensive care stay. Routine medical procedures activate
the newborns stress response system to increase cortisol secretion. Physical stressors
to the infants HPA Axis have resulted in subsequent moderate increases of cortisol
levels (Jansen, Beijers, Risken-Walraven & de Weerth, 2010). The combination of
increased cortisol levels, contributing to cell death and a failed or delayed response of
the central nervous system (CNS) results in alterations within the HPA Axis or fetal
programming (Sullivan, Hawes, Winchester & Miller, 2008).
Sullivan, Hawes, Winchester and Miller (2008), define the immediate effects of
premature birth or neonatal programming and include individual differences such as
genetic, developmental and social/care giving, which influence the neonates
behavioral and neuroendocrine response (See Figure 8). This response is heightened
Figure 8
Premature Birth: Fetal/Neonatal Programming
Figure 8. Reprinted by permission Mary. C. Sullivan. 2008-2013. In “Risk and
protection in trajectories of preterm infants: Birth to adulthood (Grant # NIH R01
NR003695-14).” Bethesda, MD, National Institutes of Health, National Institute of
Nursing Research.
or hypersensitive and contributes to the neonatal allostatic load. Long-term
exposure to repeated negative developmental stress increases the allostatic load on the
HPA Axis and if not counteracted by positive or protect factors, such as mediated by
mother-child attachment security, then adult outcomes of disease occur. Sullivan,
et al. (2008), attributes adulthood disease development to factors both positive and
negative, defined as cumulative risk and protection, which affect long-term outcomes
of functional, emotional, executive brain and work performance (See Figure 9).
In summary, early trauma with long term neurological consequences that are
dysfunctional, especially when paired with the proper timing of a stressor, at a critical
time in the development of a child, may result in health, emotional and behavioral
consequences exhibited in adulthood.
Figure 9
Cumulative Effects of Caregiving and Social Environments Over Time
Figure 9. Reprinted by permission Mary. C. Sullivan. 2008-2013. In “Risk and
protection in trajectories of preterm infants: Birth to adulthood (Grant # NIH R01
NR003695-14).” Bethesda, MD, National Institutes of Health, National Institute of
Nursing Research.
HPA Axis Function in Stress and Anxiety
Anxiety is a complex response to a stressor that includes emotional, cognitive,
behavioral and physiological responses. Diagnosed anxiety disorders, which last
longer than 6 months, affect 40 million adults age 18 and older each year (NIMH,
2009). Anxiety disorders commonly occur with mental and physical illnesses, as well
as alcohol and substance abuse. Individuals may complain of uneasiness, fearfulness
or nervousness, increased heart rate and increased respirations, to mention a few signs
and symptoms.
Walter Cannon’s well-known fight or flight response, further developed later by
Hans Selye, prepares the body to respond by increasing blood pressure, heart rate,
cardiac output and other responses as indicated in HPA functioning noted earlier
(Halter & Vascarolis, 2010). If the individual’s underlying neurological functioning
or HPA Axis functioning is dysfunctional then mediating effects, positive and
negative or cumulative protective and risks factors, will effect this response according
to the DOHaD theory. These mediating stress effects can be from a physical,
psychological, emotional, cognitive, intellectual, major life events, environmental and
social/caring interactions.
If the individual’s anxiety is transient and without dysfunction then no permanent
change will occur in the HPA Axis functioning If there is an early trauma, such as
prematurity, with long term neurological consequences that are dysfunctional, paired
with the proper timing of the stressor during critical developmental periods of the
child, then the consequences will be evident in adulthood (Turner-Cobb, 2005). In
other words, the adaptability to a stressor or anxiety rather than the initial reaction will
predict long-term outcomes.
What is known during childhood, is the relationship of low birth weight in
preterm births and subsequent psychopathology is coactive with psychiatric problems
but not necessarily medical problems (Nomura & Chemtob, 2007). Additionally
directionality of cortisol levels in childhood is known and has been determined by
their behavior of engaging or withdrawing responses (Turner-Cobb, 2005). Often a
child born prematurely will have a blunted cortisol response. A blunted cortisol
response, is defined as a failed, less intense, less concentrated or delayed cortisol
response (Bruehl, Wolf, & Covit, 2009; Sullivan, et al, 2008).
Various adult studies exist that measure cortisol levels in a variety of
psychological pathologies, emergency situations, and anxiety reduction interventions
(Harvey, Nathens, Bandiera & LeBlance, 2010; Rapaport, Schettler & Bresse, 2010;
Yu, 2010). At the other end of the life spectrum, Lanze, Mantella, Shi, et al., (2010),
report that researchers have found that one-third to one-half of elders develop
generalized anxiety disorder later in life, when aging neurological processes interfere
with brain cortex messages to the HPA Axis.
Although they are careful to report that multiple neurological pathways affect
health, the utilization of the selective serotonin re-uptake inhibitor drug escitalopram
was effective in symptom reduction and reducing cortisol levels in subjects that had
diurnal pretreatment cortisol levels above normal peak and daily total levels (Lanze,
Mantella, Shi, et al., 2010).
Elevation of cortisol levels in healthy adults has been found when the subject is
exposed to a standardized transient psychological stress test, the Trier Social Stress
Test (TSST) to trigger an acute anxiety or stress response. If a stressor or anxiety
response is elicited then the corresponding standardized timed cortisol level responses
reflect this change. A baseline diurnal cortisol level is obtained for comparison to the
stress induced cortisol response to measure reactivity of the HPA Axis. This
psychological stress induced measurement is useful to look at the level of stress or
anxiety triggered (and the HPA Axis response) and the intensity level of the cortisol
release.
Stress, coping, emotional intelligence and emotional health differences have
been found in some studies with prematurely born children. Given that the prefrontal
cortex and limbic system is part of the corticotropin releasing factor system, then
involvement of these structures and function effects will also influence emotional,
affective, appraisal and coping in the emerging adult (See Figure 10).
Summary
Structural differences in the brains of premature, low birth weight infants with
alterations continuing into adulthood have been found by researchers (Nostarti,
Murray& Hack, 2010). The concept of allostatic load and research studies related to
DOHaD theory links (Sullivan, 2008-2013): “1. Repeated infant stress responses to
prematurity and neonatal experiences with increased allostatic load. 2. The
cumulative effects of the social environments overtime with disease formation”.
Measurements of brain pathology using a variety of biomarkers, such as magnetic
resonance imaging and free saliva cortisol levels, have yielded general structural and
functional data. Salivary cortisol levels as a major endocrine marker of the HPA
activation is in wide use to measure stress responses, allostatic load, allostasis, health,
Figure 10
Stress, Coping, Prefrontal and Limbic System, HPA Axis, Cortisol, Emotional
Intelligence and Emotional Health
EMOTIONAL STRESSOR
|
APPRAISALS (Aversive)
|
_____________________________________________________________________
CORTISOL ___ ___ ___ ___ ___ ___ ___ ___ ___
| = Prefrontal Cortex & |
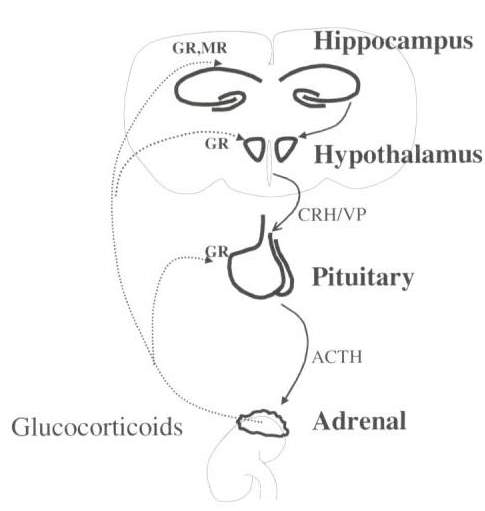 Limbic System: Sensory
Limbic System: Sensory
Cognitive & Memory |
&
COPING |
(Focus & Method)
| |
|
= ANS ——–SNS |
Increase heart rate
| |
|
| |
= CORTISOL ___ ___ ___ ___
|
|
|
_____________________________________________________________________________________________
|
|
_____________________________________________
EMOTIONAL OUTCOMES
_____________________________________________
Figure 10. Adaptation from Dorine Felder with permission, (2003), “Schematic overview of the hypothalamic-pituitary-adrenal (HPA) axis. Stress activates the HPA-axis and thereby enhances the secretion of glucocorticoids from the adrenals”. CC BY-SA 4.0 (http://creativecommons.org/licenses/by-sa/4.0)], via Wikimedia Commons. Retrieved December 15, 2016.
disease and psychiatric pathology. (Turner-Cobb, 2005). Salivary cortisol sampling
is non-invasive and easily, as well as, reliability measured.
The TSST, is another well established standardized protocol for provoking the
physiological and emotional stress responses in a laboratory setting for acute stress
reactions. Measurements of TSST cortisol stress responses, in early adulthood (age
23) allows us to examine differences in HPA Axis functioning between former
premature and full term infants and prior to later adulthood and later aging process
interactions.
Emerging adults, at Age 23, have multiple intrapersonal, interpersonal and stress
adaptability reactions to master in order to reach developmental milestones and will
require effective emotional intelligence and emotional health. Societal changes in
when emerging adults met the traditional milestone goals and the globally observed
increased risk-taking behaviors also warrant examining emerging adults coping styles.
Emerging adults coping styles to deal with stress will not only influence their current
emotional health yet will be carried with them into adulthood. Stress, coping, the
cortisol stress response, emotional intelligence, and emotional health are all involved
in obtaining developmental milestones at Age 23 for emerging adults. Results from
this study will inform us not solely of current emerging adults’ emotional health
status, yet also importantly, if there are any prematurity effects to address that
may point to risk for later adult disease.
Secondary Data Analysis
This secondary analysis is derived from the dataset of a prospective longitudinal
cohort designed study of preterm and full term infants: Risk & Protection in
Trajectories of Preterm Infants: Birth to Adulthood (Sullivan 2008-2013). The
project received full IRB approval from the University of Rhode Island, Women &
Infants Hospital and Rhode Island Hospital. The study also received a Certificate of
Confidentiality from the National Institutes of Health. The subjects (N = 213) were
born at Women & Infant Hospital between 1985-1989 and continually followed at 9
time points in research studies: 1 month, 18 months, 30 months, age 4, age 8, age 12,
age 17 and age 23. The sample retention rate at age 23 was 85% (N = 180).
The original researcher’s theoretical perspective was derived from DOHaD theory
and the purpose was to follow preterm (with ranges of gestational age and perinatal
morbidity) and full term born infants to age 23 to examine “the impact of prematurity,
medical history, and environments on achievements and deficits during young
adulthood (Sullivan, 2008)”. The original study had 3 specific aims with related
hypotheses that focused on determining the effects, relationships, and outcomes of
young adults (age 23 years old) in terms of: health (especially cardiovascular),
functional performance, emotional intelligence, executive function, work competence,
growth, neurological morbidities and psychological processes. This secondary
analysis adds an in-depth subset analysis of findings related to stress, coping, EI,
emotional health and psychiatric disorders of the infant born prematurely at age 23
(Miller & Brewer, 2003).
Compatibility of the primary data with this secondary analysis is not an issue and
will still provide information on the differences over time between 23 year olds born
pre or full term (Miller & Brewer, 2003; Yea & Niemeier, 1996). No data collection
expenses with be incurred in this secondary analysis study as did in the original
longitudinal study. The first wave of the recruited participants did not change over
time and the retention rate (85%) and those lost to attrition at age 23 (15%) remained
less than 20% allowing confidence in interpreting the differences between birth groups
(Gordis, 2009; Miller & Brewer, 2003; Yea & Niemeier, 1996).
The initial cohort was well characterized and the study procedures and
measurements were standardized and well defined. An “exposed” group of
prematurely born and a “non-exposed “ group of full term born infants comprised the
two comparison groups and were selected for birth status, neonatal illnesses, gender
and wide representation of socioeconomic status. The original researchers followed
protocols without changes in research staff resulting in minimization of personnel
effects threatening the internal validity (Miller & Brewer, 2003; Menard, 2007). As
with all longitudinal studies, all factors involved over time, are not captured yet the
original design accounted for common confounding variables associated with changes
in socioeconomic status between birth and age 23 and gender differences (Menard,
2007).
The two time points used in this secondary analysis add a distinctive period
over time and allow for identifying levels of stress adaptability, coping styles,
emotional intelligence levels and emotional health status (Singer & Willet, 2003).
Measurements included self-report, interview, observational coding, and standardized
protocols used over the course of the longitudinal study were age appropriate, and
minimized the effects of the setting and participants’ acclimation (Menard, 2007).
Furthermore, the current researcher had limited involved in the original research
nonetheless had access to the principal researchers for clarification, understanding and
information related to the study design, data, meaning and decision processes (Miller
& Brewer, 2003)
Ethical, confidentiality issues and use of the participants’ identity cleansed data
was addressed in the original study consent form at all time points and are not
accessible to this researcher (Miller & Brewer, 2003). Notwithstanding the
availability of the original dataset, the selection and in-depth understanding of the
dependent variables required extensive analysis. In addition, modeling analysis of
change variables is possible with this design (Singer & Willett, 2003). What is
unique about this secondary analysis is it begins with the identified preterm and full
term birth groups before any manifestations of emotional issues and psychiatric
disorders develop and focus on the time point of the age 23 year old participants.
Summary
This study examined all dependent variables both alone and in combination that
may influence the prematurely born emerging adult in developing emotional health
issues. Before the research plan for this study could be fully developed, a theoretical
and concept analysis of the Developmental of Health and Disease Theory, HPA Axis
functioning and Emotional Intelligence was done to clarify the concepts and constructs
and provide direction in measurement. Issues in conducting a secondary analysis
were reviewed. In Chapter 3 the secondary analysis and original study description,
sample characteristics, methodology, and data analysis plan to investigate any
differences in emotional health between the preterm and full term born emerging adult
is described.
CHAPTER 3
Methodology
This study is a secondary analysis of a larger longitudinal study aimed at
determining the effects of prematurity, risks and protective processes on adult
trajectories and health outcomes at age 23. The original study’s theoretical
foundation is the Developmental Origins of Health and Disease (DOHaD) and the
variable measurements used are consistent with the purpose of this secondary analysis.
This secondary study is a descriptive correlational design of the effect of premature
birth and its relationship to stress, coping, emotional intelligence, emotional health and
the stress response of neuroendocrine functioning at age 23. In this chapter, sample
and neonatal demographics, self-report measures of stress, coping and emotional
intelligence, assessment of emotional health, and timed measures of salivary cortisol
through a standardized laboratory social stress paradigm, the Trier Social Stress Test
(TSST) are defined. The study procedures and data analysis plans are outlined.
Research Design
The University of Rhode Island, Office of Research Integrity, determined this
secondary data analysis, did not require Institutional Review Board (IRB) oversight:
# 910108-1 (See Appendix L).
Sample
The infant participants were born at Women’s and Infants Hospital in Rhode
Island between 1985-1989, continually followed in a series of research studies
supported by the National Institutes of Health (Lester, 1985; McGrath, 1989, 1994,
1998, 2003; Sullivan, 2008 – 2013. The infant sample included 213 infants in a
5-group design of: (1) full term healthy infants (FT), (2) preterm infants without
neonatal illness (HPT), (3) preterm infants with neonatal medical illnesses (MPT),
(4) preterm infants with neonatal neurological illness (NTG) and (5) preterm infants
with small for gestational age (SGA) with and without neonatal illness, (Sullivan,
2008-2013). The original racial and ethnic composition of the 213 sampling,
consisted of 105 females and 108 males, and was reflective of the population and
geographical location in Southeastern New England from 1985 to 1989 (Sullivan,
2008-2013). This original sampling included varied degrees of neonatal morbidity
in preterm birth. The study maintained a 97% retention rate from age 4 to 23 years
(Sullivan, 2008-2013). At age 23 years, 180 subjects were recruited for participation
in the 10th longitudinal follow-up study with a retention rate from birth of 85%, and
96% from the prior age point of 17 years. Two time points, birth and age 23 years,
the 10th wave of this longitudinal study comprised the sample for this study.
The data (Appendix Measurements) utilized for this study will consist of neonatal
data from the original five groups and demographics. Age 23 years data are, the
self-report measures of the Daily Hassles (DHS-R) for stress, Coping Response
Inventory (CRI-A) for coping styles, the Bar-On Emotional Quotient Inventory
(Bar-On EQi) for emotional intelligence, emotional health status from the Adult Self
Report (ASR) and salivary cortisol levels collected according to the established
protocol from the Trier Social Stress Test (TSST).
The neonatal sample inclusion and exclusion criteria as well as the characteristics
of 5-group design are well described (Sullivan, 2008-2013; Winchester, Sullivan,
Roberts & Granger, 2016). For this study, inclusion criteria included the ability to
participate and complete the study protocol and measures. Any 23-year old
participant with severe medical problems, such as cerebral palsy with wheelchair
assist, or low intelligence with or without physical limitations was excluded. Females
who were pregnant, tested positive using urine pregnancy screening, or <8 weeks
post – partum were excluded from the original data collection. Additionally any
23-year old young adult with positive urine testing for substance use was excluded.
Measurements
The following measurements are proposed for the current study.
Demographic Data
Demographic data included neonatal birth data at age 23 including the
Hollingshead Four Factor Index of Social Status (HH), (Holmes & Rahe, 1967). HH
was used to estimate the socioeconomic status of unmarried individuals, female and
male heads of households and families (Hollingshead, 1977; Gottfried, 1985). It is
widely used in medicine and public health to differentiate socioeconomic status
(Adams & Weakliem, 2011). The four factors examined consist of: education,
occupation, sex/gender and marital status that are used to derive a mathematical
estimate of social status (Hollingshead, 2011).
The occupation scale is scored between 1 and 9, nine being the most highly
regarded occupations and one being less highly regarded careers. Examples of
occupations which would receive a score of nine are architects, lawyers and
physicians, while occupations that would earn a score of one are janitors, dishwashers
and personal attendants. A seven-point scale is employed to determine educational
status. A seven indicates the completion of a graduate degree or higher while a one
represents completion of less than a seventh grade education. To acquire a social
status score the occupation score is multiplied by 5 and the education score is
multiplied by 3 (Hollingshead, 1977). In families with two gainfully employed
persons the total score is divided by 2 to obtain a social status score. The range of
computed social status scores (8-66) are then divided into five categories of: lower
(8-19), lower-middle (20-29), middle (30-39), upper-middle (40-54) and upper
(55-66), (Hollingshead, 1975).
The Hollingshead Four Factor Index of Social Status is used as a benchmark to
compare other measures of socio-economic status (Adams, J., & Weakliem, D., 2011).
The Hollingshead reliability correlates with other indices of SES with ranges of
.73-.89 (Cirino, Chin, Sevcik, Wolf, Lovett & Morris (2002). The social scores
achieved are considered the best valid measure of socioeconomic differentiation
available (Cassidy, Drotar, Ittenbach, Hottinger, Wray, Wernovsky, Newburger,
Mahoney, Mussatto, Cohen, & Marino, 2013; Adams, J., & Weakliem, D., 2011).
Stress
Stress (psychosocial) measurements include everyday and major life
experiences as captured by the Daily Hassles Scale-Revised (DHS–R). The
DHS–R, developed by Kanner, Coyne, Schaefer & Lazarus, (1981), focuses on
everyday stressors instead of major stress life events and psychological and somatic
symptoms (Holm & Holroyd, 1992). Measures of daily life hassles in 53 items (e.g.,
time alone, your spouse, your health) on a 4-point scale, ranging from “none or not
applicable” to a “great deal.” The item scores are summed to give a score for the
overall severity of hassles, ranging from 0-159. Internal consistency was .93-.97
over 2 years. Mean day-to-day correlation was .77 and mean monthly correlation
was .82. Daily hassles severity is related to depression, anxiety, PTSD and role
stress. The DHS–R has been previously used in studies with preterm born children
(Msall & Park, 2008).
Coping
The Coping Response Inventory-Adult Form (CRI–A) measured coping
responses, at Age 23 (Billing & Moss, 1981; Moos, 1995; Moss & Holahan, 2003).
The CRI-A form, developed by Rudolf Moos, is a 48-item self-report inventory
measuring cognitive and behavioral responses to stress. It measures coping
orientation focus (approach or avoidance) and methods of coping used (cognitive or
behavioral)
The CRI–A is appropriate for use in both healthy adults 18 years of age and
older, and those with psychiatric, substance abuse and medical diagnoses. The
instrument may be administered in structured interview or self- report format. The
participants select and describe a recent stressor (within the last year) and use a
four-point scale varying from “not at all” to “fairly often” to rate their reliance on each
of the 48 coping items. Eight types of approach and avoidance coping responses are
derived from the items. Approach responses include logical analysis, positive
appraisal, seeking guidance and support, and problem solving. Avoidance responses
include cognitive avoidance, acceptance or resignation, seeking alternative awards,
and emotional discharge. Within each of the approach and avoidance responses, the
first two scales are representative of cognitive coping strategies and the third and
fourth scales of behavioral coping strategies (Moos, 1993).
Additionally, ten appraisal items assess if the stressor was expected, viewed as a threat or challenge, the perceived cause and if resolution has occurred. Participants respond to questions aimed at examining the context of the stressor using a
four-point scale varying from “definitely no” to “definitely yes” (Moos, 1993).
The CRI-A is interpreted using T-scores, with possible T-scores ranging from 20 to 80 + with a mean of 50 and a standard deviation of 10. A T-score of < 34 is considerably below average and a score of > 66 is considerably above average. Internal consistencies range from 0.61 to 0.74 for males and 0.58 to 0.71 for females. Cognitive avoidance internal consistency as measured by Cronbach’s alpha is .71 and emotional discharge is .60. Avoidance coping “across time (1-year stability = .56;
6-year stability = .51) and across life domains (ie., interpersonal, health, and financial stressors), has been found to be stable (Holahan, Moos, Holahan, et al., 2005). “ Test-retests alphas showed moderate stability over 12 months (average
r = 0.45 for males and 0.43 for females). Content and face validity was built into the CRI-A by formulating definitions of specific domains, preparing items to fit the construct definitions, and selecting items that were conceptually and empirically related to a dimension. Reliability and validity have been extensively researched and found to be adequate (Moos, 1993 & 2004).
Emotional Intelligence
The Bar-On Emotional Quotient Inventory (Bar-On EQi) was used to
measure the emotional intelligence of all participants. The Bar-On EQi is a
self-report measure of emotional and social behaviors and the participants potential
to deal with daily environmental demands and pressures (Bar-On, 2002 & 2006;
Sullivan, 2008). It has been used world-wide in a variety of settings with diverse
populations and translated into 30 languages since being developed in the 1980’s
(Bar-On, 2006). The Bar-On EQi contains 133 items, on a 4-point Likert-like
scale (ranging from very seldom to true), resulting in 5 composite scales and 15
subscales (Sullivan, 2008; Bar-On, 2006). The 5 composite scales are:
intrapersonal, interpersonal, adaptability, stress management and general mood
(Bar-On, 2006)”. The intrapersonal scale measures self-awareness and
self-expression as a composite assertiveness, independence and self-actualization
subscales. The interpersonal scale measures social awareness and interpersonal
relationships as a composite score of the social responsibility and interpersonal
relationships (“the establishment of mutually satisfying relationships and relating well
with others”) scales (Bar-On, 2006). Stress management measures emotional
management and regulation as a composite score of the stress tolerance and impulse
control subscales. The adaptability score measures change management as a
composite score of the reality testing, flexibility and problem solving. The general
mood composite score measuring self-motivation is derived from the subscales of
optimism and happiness. Finally an overall total emotional quotient score is
generated.
The 133 items are rated on a five-point Likert-type scale with choices ranging
from “very seldom” or “not true” to “very often true” or “true”. The raw scores are
converted into standard scores with a mean of 100 and standard deviation (SD) of 15.
The higher the score the more potential for effective emotional and social functioning
and the prediction for meeting daily demands and challenges (Bar-On, 2006).
The Bar-On EQi questionnaire has a built in validity correction factor that
adjusts for response bias. Internal consistencies range from .69 – .96 with all
composite scales correlate highly with the total EQ-I scores (.67 to .93), (Dawda &
Hart, 2000). Test-retest reliability at six months ranges from .72 to .80 (Bar-On,
2006). Ten subscales from a confirmatory factor analysis are the strongest measures
of the construct: self-regard, interpersonal, impulse control, problem solving,
emotional self-control, “emotional self-awareness, flexibility, reality testing, stress
tolerance, assertiveness and empathy (Bar-On, 2006).” The remaining 5 subscales
are facilitators of emotional and social intelligent behaviors: independence,
self-actualization, social responsibility, optimism and happiness. The Bar-On EQi
has been extensively researched and validated with evidence strongly supporting
construct, divergent, discriminant, criterion, and convergent and predictive validity.
Emotional Health
The Adult Self-Report (ASR) was used to determine emotional health. The ASR
for ages 18-59 is extensively researched and used widely in research studies for well
over twenty years (Achenbach, 2003). The ASR assesses social competence and
behavior problems in adults ages 18-59. The participant completes the ASR and
report their own functioning, problems and substance use. It provides normative
scales for functioning, syndromes, substance use, internalizing, externalizing and total
problems (ASEBA, 2011). The syndrome scales are then profiled to international
expertly derived Diagnostic and Statistical Manual of Mental Disorders Fourth
Edition Text Revision (DSM IV-TR) oriented scales (Archenbach, 2003).
The ASR (2003) is composed of data relating to friends, spouse or partner, family,
job, education and a list of self-descriptors. The descriptor list contains 126 items
rated on a 3-point scale consisting of “ not true, somewhat, or sometimes true and
very true or often true”. Raw scores are converted in t – scores are categorized into
clinical risk screening ratings of normal (t = <59), borderline (t = 60-63), and clinical
(t = 64 and above). Classification parameters resulted in true positives
(sensitivity) = 80%; true negative (specificity) = 95%; false positives = 20%; false
negatives = 5%.
Category scores are related to DSM IV-TR disorder criteria. Internalizing
behaviors include anxiety, depression and withdrawn behaviors while externalizing
behaviors include aggression, rule breaking and intrusive behaviors. The
DSM-oriented problem scales are depressive; anxiety problems; somatic; avoidant
personality; AD/H and antisocial personality.
Reliability is excellent: 1-week test-retest correlations were .80 – .90, 2 years
was .69 with none below .71. Internal consistency range was .78 – .85. Discriminant
validity was demonstrated in the referred and non-referred samples and with
DSM IV-TR categories.
Stress Reactivity
The stress reactivity responses were measured by the Trier Social Stress Test
(TSST). The TSST, developed by Kirschbaum, is a standardized protocol for
inducing stress to subjects in studies and deliberately activates the HPA axis response
(Kirschbaum, 2010; Kirschbaum, Pirke & Hellhammer, 1993). It was used in this
study to assess physiological reactivity to what the participant perceives as a
challenging situation which has the potential for being negatively judged by others
(Kudielka, 2008; Sullivan, 2008 – 2015). In addition to invoking reports of negative
mood changes and increased anxiety, the HPA Axis response of endocrine,
immunological and other biological markers have been well documented (Stolerman,
2009). It is widely used and involves a well-scripted task the participant is asked to
engage in hypothetically while others are evaluating their verbal response. The task
consists of a brief preparation period (10 minutes), a test period where the participant
delivers a speech for a mock interview (5 minutes) and finally a period of calculating
mental arithmetic (5 minutes) in front of an audience. While completing the tasks the
participants are also being video recorded to later assess their behaviors while under
stress. In the original study their behavioral presentation will be evaluated according
to pre-established definition levels of: humor, anxiety, non-verbal but otherwise
engaged, defensive, aggressive, scorn, frustration and distraught.
Salivary cortisol samples are collected at the following intervals: prior to the task
(baseline), 15, 30, 45, 60, 75 and 90 minutes after the task has started (Sullivan,
2008-2013). A mandatory part of the protocol is participants are debriefed after
completion of the test (Kirschbaum, 2010). The TSST has been used with children,
adults, healthy subjects and clinical populations. It is among one of the few tests that
assess both behavioral and psychobiological responses to situations that are perceived
as uncontrollable and socially threatening (Kudielka, 20008; Dickerson & Kemey,
2004).
HPA Axis Biomarker: Salivary Cortisol
Salimetrics, Inc., Expanded Range High Sensitivity (ERHS) Salivary Cortisol
Enzymes Immunoassay Kit for research was used to collect samplings during the
TSST (Salimetrics, Inc., 2008). Sensitivity and specificity of the Salivary Cortisol
Enzyme Immunoassay is excellent, as well as, a widely used solid technology, and the
“gold standard among researchers. The laboratory procedures include duplicate
assays for each cortisol sample so that each saliva sample is tested twice on the assay
plate. This renders two data points per sample and a mean for each sample tested in
duplicate. Duplicate assays minimize the potential of with-in subject variability.
Each assay captures the full range of salivary cortisol levels (0.003 to 3.0 ug/dL) while
using only 25 uL of saliva per test (Salimetrics, Inc., 2008). The lower limit of
sensitivity was determined by interpolating the mean minus 2 standard deviations
(SDs) for 10 sets of duplicates at 0 ug/dl standard. For sensitivity, the minimal
concentration of cortisol that can be distinguished from 0 is < .003 ug/dL. The
correlation between saliva (Salimetrics ERHS Salivary Cortisol EIA) and serum
(Diagnostic Systems Laboratory) was highly significant (r = .91, p = .0001). During
testing, a potential hydrogen (ph) indicator alerts if cortisol levels are artificially
inflated or lowered (< 3.5 or > 9.0); possible blood contamination is screened; and
temperature is controlled. Specificity of antiserum varies but is excellent. The EIA
is accurate in diagnosis of Cushing Syndrome (Raff, Homan, & Skoner, 2003; Lucke,
Loucks & Berga, 2007). Sensitivity/Specificity of 100 %/95 % was reported for
salivary cortisol to distinguish diagnosis of Cushing’s syndrome and obesity in an
age-matched sample of children (Castro, Elias, Martinelli, Antonnini, Santiago &
Moreira, 2000). Various adult studies exist that measure cortisol levels in a variety of
psychological pathologies, emergency situations, and anxiety reduction interventions
(Harvey, Nathans, Bandiera & LeBlance, 2010; Rapaport, Schettler & Bresse, 2010).
In the primary study, a careful research protocol was followed. A foam oral
swab was used to collect saliva and placed under the participant’s tongue for 2
minutes. Approximately 1 mL. of saliva saturated the foam swab and then it was
inserted into a labeled collection tube and stored in a freezer. The saliva samples
were placed into a cryostorage box with a minimum of 5 lbs. of dry ice and shipped
via Federal Express Priority for analysis by Salimetrics, Inc. Samples were typically
submitted to Salimetrics quarterly (every 3 months) but more frequently when
necessary. Shipping instructions according to www.salimetrics.com were followed.
Once analyzed, specimen data were entered into a spreadsheet by Salimetrics, Inc.
and reported to the Principal Investigator via e-mail in the form of an Excel file with
two values for each saliva sample and the mean in the form of a concentration (e.g.,
cortisol = 0.652 ug/dL). Saliva samples were discarded according to Pennsylvania
Department of Environment Protection regulations 30 days after testing was
completed. Data from the log were entered into MS Excel by study staff. The only
identifier between the participant and the saliva sample was a predetermined label
provided by Salimetrics, Inc., who had no access to data to link the sample to the
participant. It was the responsibility of the research staff to link the participant’s
unique identification number with the Salimetrics predetermined label.
Summary
Data for the proposed study include neonatal and demographic data from infancy
and self – report questionnaires, 8 sequential salivary cortisol samples from the TSST
standard laboratory protocol from the same participants at age 23 years. The
measures are well developed with good psychometric values. Questionnaire scoring
and subscale information are provided in the Appendix Measurements
Procedure
Researcher
In the study, the researchers were kept blinded to all identifying information
which was coded by the primary study staff. The coded database was not associated
with identifying information. The anonymous complete dataset for the study was
provided by the project director.
Recruitment
The infancy sample was recruited during the mother’s post-partum stay or during
the infant NICU stay. The full term infants were identified during the post-partum
and in the same time frame as the preterm infants. The criteria for recruitment were
neonatal diagnoses, birth weight < 1850 grams (4 pounds), maternal history (no
history of mental illness), and English as a primary language. Parent(s) were then
invited to participate by research nurses. Fewer than 10% of the parent(s) declined
participation.
Neonatal Group Criteria was: (1) full term healthy infants (FT); (2) preterm
infants without illness (healthy preterm group: HPT); (3) preterm infants with medical
illness (bronchopulmonary dysplasia, respiratory distress syndrome, necrotizing
enterocolitis and sepsis: MPT); (4) preterm infants with neurological illness
(meningitis, hydrocephalus, and grade 3 or 4 intraventricular hemorrhage: NPT); and
preterm infants who were small for gestational age (SGA). Additionally specific
protocols for neonatal diagnostic labeling were used. The range of premature infants
in weeks and grams were from 28.3 to 40 weeks gestational age and 1149 (2.5 lbs.) –
3420 (7.5 lbs.) grams in weight. Socioeconomic status, incorporating both maternal
and paternal education and occupation, was measured with the Hollingshead Four
Factor Index.
Infants were followed in a series of research studies at ages 18 months, 30
months, 4 years, 8 years, 12 years, and 17 years. At age 23, the original researchers
who had worked with the participants for more than 10 years, made recruitment
contact again. Sample retention was high with 96% of the sample from age 17 years
and 85% of the birth sample participating at age 23 years. The research protocol
included a home visit and hospital research laboratory visit.
Demographics
At age 23, demographic information was updated to include name, address, home
and cell telephone numbers, e-mail address, social security number, marital status,
education level/history, occupation/history, source(s) of financial support, lists of
people living in home, pregnancies (for female subjects) and number of children,
closet relative information, primary care provider information, and use of medical and
community support services. The participant also filled out his or her own
Hollingshead Four Factor Index of Social Status.
The Daily Hassles Scale-Revised (DHS-R), the Coping Response Inventory
(CRI-A), the Bar-On EQi and the Adult Self-Report (ASR) were administered to each
participant, as part of the larger study protocol of tests and questionnaires, during their
first laboratory visit. Laboratory visits were scheduled according to standardized time
periods. Each participant followed the same schedule or sequencing of
questionnaires, food breaks and examinations throughout the specified time period
allowing for consistency in protocol and comparison between participants. This
battery of tests was administered after completion of the history and physical in a
small private room free from distractions. The research assistants monitored, timed
and administrated the sequencing of tests according to study protocols.
TSST Protocol
The Trier Social Stress Test (TSST) followed standardized and extensive protocols
relating to timing during the day, timing with other testing and testing protocols.
Levels of cortisol are heightened in the morning and decline throughout the day. To
reduce the potential of varied cortisol levels among subjects, administration of the
(TSST) was standardized to 1 pm for all participants. Upon arrival the research nurse
(RN) greeted the participant, explained the laboratory protocol, confirmed consent and
addressed questions. To avoid confounders in possible stimulation of the HPA axis,
the RN inquired about health-related limitations (colds, flu), physical activity,
smoking, medications, large meals, and hormonal treatments within the last 2 hours.
The RN had informed participants of these restrictions when the testing was
scheduled. Participants were not informed in great detail about the exact procedure of
the TSST. The RN inquired about the participant’s ideal occupation as this was
necessary information for the speech segment of the TSST protocol. A baseline
salivary cortisol sample was collected 20 minutes after arrived (and the time noted)
followed by the TSST.
The participants were escorted to an assessment room and told there would be two
parts to this segment: (1) mock job interview and (2) arithmetic problem. All scripts
were followed verbatim. For the mock job interview, the participant was instructed
by the researcher with a scripted standardized comment. The participant was given
10 minutes to prepare for the interview and informed that no notes could be used and
they needed to make an impression on the committee (composed of 4 research
assistants) who would decide on the acceptance of the application.
The mock job interview was allowed 5 minutes, only one RA would talk and
direct the participant and the rest would be silent, with focused eye contact and a
serious demeanor that excluded any non-verbal encouragement. A dummy video
camera was set up for the mock interview and the participant was asked to “please
step behind this line, and begin your speech.” All research assistants followed
protocols for their roles, behavior, eye contact, facial expressions and speech. If there
was a pause in the speech, then at 20-seconds the participant was told: “You still have
time, please continue.” Should there be another pause and the participant has
nothing to add then the RA will ask a standardized set of questions until the 5-minute
time period ended. At the end of the job interview time the RA announces that the
second part of the test will begin and states it had nothing to do with the job interview.
The verbal instructions to the participant for the arithmetic test is also scripted and
in part includes:
“We ask you to count backwards to 0 in 13 number steps, starting at 1687.
It is important to do it fast and correctly. Should you miscalculate, you
will be told to start again at 1687. Any questions? Please begin.”
During this time the RA made notes on paper for errors in calculations. If the
participant miscalculates, the RA will respond with “Error. 1687.” After 5-minutes
of mental arithmetic, the RA stopped the TSST.
The second cortisol sample was collected 20 minutes after the TSST. In the
interim, the RN conducted the health history interview. After the collection of the
cortisol sample there was a break and then additional questionnaires were
administered and collected. The third cortisol sample was collected after the
questionnaires were completed, approximately 30 minutes after the collection of the
second sample (50 minutes after the TSST). The RN then begin the debriefing of the
TSST with:
“The first thing I’d like to tell you is that the job interview speech and the
arithmetic part were supposed to be difficult. We did this to elicit a stressful
situation for you. When people encounter stressful events, their bodies respond
with an accelerated heart rate and the body produces cortisol. We will be
measuring your cortisol through your saliva. We were not really recording
audio or video for preverbal stress or behavioral analysis. Also, the judge is
actually one of our research assistants. Let me introduce you to him/her.”
After, the debriefing, a healthy snack was given and further assessment inventories
were administered. The physical examination followed and further salivary cortisol
samples were collected at 60, 75 and 90 minutes.
Summary
All measurements representative of the dependent and independent variables to be
utilized in this secondary analysis have been reviewed along with the original
study procedural protocols. Use of this data, from the original measurements with
good psychometric prosperities, remains a strong fit to the aims of this study despite
the longevity of the original study design.
Analysis
All data was analyzed using the IBM SPSS Statistics Standard Grad Pack
(SPSS), Version 22 descriptive statistics. The SPSS is used widely in social science
research to obtain descriptive statistics (mean, standard deviation, range), graphic
depiction, and hypothesis testing (Chi Square, ANOVA, ANCOVA, MANOVA and
MANCOVA.
First frequency statistics were performed for each variable. The frequency
and pattern of missing data were reviewed. Missing data imputation was considered
when > 10 % data were missing. Distribution skewness, kurtosis, box-plots were
examined and transformations considered when needed. Correlations were examined
between all dependent variables. Correlations > .80 were considered to behighly
correlated and decisions were made to use one variable (FGSE, 2016). The
significance level wasp < = .05. Analysis of Variance (ANOVA) was used to
determine any variations within and between the groups (LoBiondo-Wood & Haber,
2010) in all self-report variables. AUCg was used with the cortisol endocrine data
as a measurement of hormonal output (Fekedulegn, et. al., 2007). The AUCg is
the total area under the plotted curve of all the multivariate measurements and allows
for identification of the differences between the single measurements and the distance
of these measurements from ground (Spence, Cotton, Underwood & Duncan, 1976).
Measurements from ground (see Figure 11) take into consideration the distance from
zero instead of baseline data points and allows for total salivary cortisol response
comparisons between participants. (Fekedulegn, et. al., 2007). Finally, the level of
effect power range recommended to reduce any Type I (is effect when there is
none) or II (no effect when there is) error at the 0.05 significance criterion is
0.80 – 0.95 (Lakens, 2013). The study’s’ power was calculated at the 0.80
significance criteria.
Figure 11
Area Under the Curve with Respect to Ground (AUCg)
Figure 11. From: Catherine Raymond, Marie-France Marin, Anne Hand, Shireen Sindi, Robert-Paul Juster, and Sonia J. Lupien, “Salivary Cortisol Levels and Depressive Symptomatology in Consumers and Nonconsumers of Self-Help Books: A Pilot Study,” Neural Plasticity, vol. 2016, Article ID 3136743, 12 pages, 2016. Figure 4,p 9. doi: 10.1155/2016/3136743 http://doi.org/10.1155/2016/3136743 Retrieved December 15, 2016. This is an “open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.”
Aims and Hypotheses
Aim 1: Compare effect of prematurity on stress, coping, emotional intelligence
and emotional health. Compare independent categorical variable of birth groups with
the dependent continuous variables: DHS summed scores ranging from 0-159 for
severity of stress, the CRI-A mean scores ranging from 20-80 + with M 50 (SD 10)
for avoidance coping, the Bar-On EQI total mean score of 100, (SD 15) for
emotional intelligence effectiveness and the ASR mean score of > 60 for risk to
emotional health.
Hypothesis 1. Higher self -reported stress scores, higher use of avoidance
coping styles, lower emotional intelligence scores and more emotional health
disorders will be found for the adults at age 23 years born prematurely compared to
the term-born adults. Hypothesis 1 will be significant if DHS-R total scores are
higher, CRI-A avoidance t-scores are higher, EQi total scores are lower, and ASR
scores are higher for the premature groups.
Aim 2: Compare the salivary cortisol response between premature and full-term
born infants in the social stress paradigm of the TSST. Descriptive statistics
including line graphs by groups will be examined first. Analysis of Variance
(ANOVA) will be used to determine differences in salivary cortisol responses as
measured by AUCg and at 6 sample times from the TSST paradigm at 15, 30, 45, 60,
75 and 90.
Hypothesis 2. Adults at age 23 who were born prematurely will have a prolonged
stress recovery period for the TSST. Hypothesis 2 will be significant if the AUCg
mean is higher during the stress recovery period for TSST in the prematurely born age
23 year old adult.
Aim 3. Examine the relationship between effect of emotional health and on the
stress recovery period of the TSST measured in salivary cortisol. Three levels of
emotional health (normal > 59, borderline 60 – 63, and clinical > 64) as measured by
the ASR will be examined for the salivary cortisol samples across 6 sample times.
Descriptive statistics including graph lines by groups will be used followed by
ANCOVA where the effects of prematurity and gender will be controlled to
understand whether cortisol AUCg and slopes differ due to emotional health.
Hypothesis 3. The stress recovery period for adults at age 23-years with
emotional health problems will be prolonged compared to adults without emotional
health problems (as determined by ASR t-scores) when prematurity is controlled.
Summary
The measurements used for this secondary analysis are consistent with the
aims of the primary study. Measurements and procedures for all dependent and
independent variables were reviewed. The measures have demonstrated good
psychometric properties. In the original study, the research team developed and
trained on the procedure protocols. Reliability between team members in the protocol
were consistently assessed and were >/= 90 %. The design of this study allows for
correlational and multivariate modeling. The use of neonatal data enables predictive
analysis.
Tags: Custom Homework Writing Help & Assignment Answers Service, Do My Homework Fast App, Help with all Assignment shark essay writing service, Homework assignments custom writings affordable servicesYou Want The Best Grades and That’s What We Deliver
Our top essay writers are handpicked for their degree qualification, talent and freelance know-how. Each one brings deep expertise in their chosen subjects and a solid track record in academic writing.
We offer the lowest possible pricing for each research paper while still providing the best writers;no compromise on quality. Our costs are fair and reasonable to college students compared to other custom writing services.
You’ll never get a paper from us with plagiarism or that robotic AI feel. We carefully research, write, cite and check every final draft before sending it your way.