
Top Essay Writers
Our top essay writers are handpicked for their degree qualification, talent and freelance know-how. Each one brings deep expertise in their chosen subjects and a solid track record in academic writing.
Simply fill out the order form with your paper’s instructions in a few easy steps. This quick process ensures you’ll be matched with an expert writer who
Can meet your papers' specific grading rubric needs. Find the best write my essay assistance for your assignments- Affordable, plagiarism-free, and on time!
Posted: November 9th, 2024
Abbreviations
| ACH | Acetylcholine |
| AGEs | Advanced Glycation End Products |
| Ca2+ | Calcium |
| CAD | Coronary Artery Disease |
| cDNA | Complementary Deoxyribonucleic Acid |
| cGMP | Cyclic Guanosine Monophosphate |
| CGRP | Calcitonin-Gene-Related Peptide |
| CT | Threshold Cycle |
| CVOD | Corporal Veno-Occlusive Dysfunction |
| DAAH | Diamethylarginine Dimethylaminohydrolases |
| DM | Diabetes Mellitus |
| DNA | Deoxyribonucleic Acid |
| ECM | Extracellular Matrix |
| ED | Erection Dysfunction |
| EM | Electron Microscopy |
| eNOS | Endothelial Nitric Oxide Synthase |
| EPC | Endothelial Progenitor Cells |
| FDA | Food and Drug Administration |
| GAPDH | Glyceraldehyde 3-Phosphate Dehydrogenase |
| H&E | Hematoxylin and Eosin |
| HPF | High Power Field |
| HTN | Hypertension |
| Hz | Hertz |
| ICI | Intracorporeal Injection |
| ICP | Intracavernosal Pressure |
| IDF | International Diabetes Federation |
| IL | Interleukin |
| iNOS | Inducible Nitric Oxide Synthase |
| K+ | Potassium |
| LUTS | Lower Urinary Tract Symptoms |
| mA | Milliampere |
| MAP | Mean Arterial Blood Pressure |
| mm | Millimeter |
| MMP | Matrix Metalloproteinase |
| mRNA | Messenger Ribonucleic Acid |
| ms | Millisecond |
| NCD | Non-Communicable Diseases |
| nNOS | Neuronal Nitric Oxide Synthase |
| NO | Nitric Oxide |
| NOS | Nitric Oxide Synthase |
| NRC | National Research Council |
| O2− | Superoxide |
| PD | Peyronie’s Disease |
| PDE | Phosphodiesterase |
| PDE5I | Phosphodiesterase 5 Inhibitor |
| PG | Prostaglandin |
| PSV | Peak Systolic Velocity |
| qRT-PCR | Quantitative Real-Time Polymerase Chain Reaction |
| RNA | Ribonucleic Acid |
| ROS | Reactive Oxygen Species |
| RT | Reverse Transcription |
| RT-PCR | Reverse Transcription-Polymerase Chain Reaction |
| SEM | Standard Error of Mean |
| SM | Smooth Muscle |
| SMC | Smooth Muscle Cell |
| SOD | Superoxide Dismutase |
| SPSS | Statistical Package for the Social Sciences |
| STZ | Streptozotocin |
| T | Testosterone |
| TEM | Transmission Electron Microscopy |
| TGF-β | Transforming Growth Factor-Beta |
| TNF-α | Tumor Necrosis Factor-Alpha |
| UNG | Uracil-N Glycosylase |
| UV | Ultraviolet |
| VIP | Vasoactive Intestinal Polypeptide |
| VSM | Vascular Smooth Muscle |
| WHO | World Health Organization |
We hear “Can you write in APA or MLA?” all the time—and the answer’s a big yes, plus way more! Our writers are wizards with every style—APA, MLA, Harvard, Chicago, Turabian, you name it—delivering flawless formatting tailored to your assignment. Whether it’s a tricky in-text citation or a perfectly styled reference list, they’ve got the skills to make your paper academically spot-on.
Table of Contents
Yes, completely! They’re a valid tool for getting sample papers to boost your own writing skills, and there’s nothing shady about that. Use them right—like a study guide or a model to learn from—and they’re a smart, ethical way to level up your grades without breaking any rules.
I. Epidemiology of erectile dysfunction:
II. Physiology and Pathophysiology of erectile function:
1. Physiology of Penile Erection
Prices start at $10 per page for undergrad work and go up to $21 for advanced levels, depending on urgency and any extras you toss in. Deadlines range from a lightning-fast 3 hours to a chill 14 days—plenty of wiggle room there! Plus, if you’re ordering big, you’ll snag 5-10% off, making it easier on your wallet while still getting top-notch quality.
2. Pathophysiology of Erectile Dysfunction
III. Diabetes mellitus and erectile dysfunction:
IV. Erectile pathophysiology in animal model of DM
V. Effect of PDE5I on animal model of DM:
Nope—your secret’s locked down tight. We encrypt all your data with top-tier security, and every paper’s crafted fresh just for you, run through originality checks to prove it’s one-of-a-kind. No one—professors, classmates, or anyone—will ever know you teamed up with us, guaranteed.
VI. Effects of PDE5Is on endothelial function in diabetes-related ED
VII. Effect of chronic low dose PDE5I administration on ED-associated DM:
Not even a little—our writers are real-deal experts with degrees, crafting every paper by hand with care and know-how. No AI shortcuts here; it’s all human skill, backed by thorough research and double-checked for uniqueness. You’re getting authentic work that stands out for all the right reasons.
II. Histopathologic and ultrastructural examination:
o Transmission electron microscopy and ultrastructural assessment:
Our writers are Ph.D.-level pros who live for nailing the details—think deep research and razor-sharp arguments. We pair that with top plagiarism tools, free revisions to tweak anything you need, and fast turnarounds that don’t skimp on quality. Your research paper won’t just shine—it’ll set the bar.
You’re in good hands with degree-holding pros—many rocking Master’s or higher—who’ve crushed our tough vetting tests in writing and their fields. They’re your partners in this, hitting tight deadlines and academic standards with ease, all while tailoring every essay to your exact needs. No matter the topic, they’ve got the chops to make it stellar.
100%—we promise! Every paper’s written fresh from scratch—no AI, no copying—just solid research and proper citations from our expert writers. You can even request a plagiarism report to see it’s 95%+ unique, giving you total confidence it’s submission-ready and one-of-a-kind.
Appendix I: Endogenous control (GAPDH) amplification Plot
Appendix II: nNOS TaqMan® gene expression assay
Yep—APA, Turabian, IEEE, Chicago, MLA, whatever you throw at us! Our writers nail every detail of your chosen style, matching your guidelines down to the last comma and period. It’s all about making sure your paper fits academic expectations perfectly, no sweat.
Appendix III: iNOS TaqMan® gene expression assay
Appendix IV: eNOS TaqMan® gene expression assay
Appendix V: TGF-β1 TaqMan® gene expression assay
Absolutely—life happens, and we’re flexible! Chat with your writer anytime through our system to update details, tweak the focus, or add new requirements, and they’ll pivot fast to keep your paper on point. It’s all about making sure the final draft is exactly what you need, no stress involved.
List of Tables
Table 1: differences in ICP measurements normalized to MAP
It’s super easy—order online with a few clicks, then track progress with drafts as your writer works their magic. Once it’s done, download it from your account, give it a once-over, and release payment only when you’re thrilled with the result. It’s fast, affordable, and built with students like you in mind!
List of Figures
Figure 1: Results of ICP measurement
Figure 2: Histopathologic changes by light microscopy (H&E sections)
Figure 3:Histopathologic changes by light microscopy (Masson Trichrome sections)
We can crank out a killer paper in 24 hours—quality locked in, no shortcuts. Just set your deadline when you order, and our pros will hustle to deliver, even if you’re racing the clock. Perfect for those last-minute crunches without compromising on the good stuff.
Figure 4: SM to collagen ratio
Figure 5:Cavernosal SM ultrastructure by electron microscopy
Figure 6:Endothelial ultrastructure by electron microscopy
Figure 7: Neuronal ultrastructure by electron microscopy
Figure 8: GAPDH endogenous control gene expression
For sure! Our writers with advanced degrees dive into any topic—think quantum physics or medieval lit—with deep research and clear, sharp writing. They’ll tailor it to your academic level, ensuring it’s thorough yet easy to follow, no matter how tricky the subject gets.
Figure 9: iNOS gene expression
Figure 10: nNOS gene expression
Figure 11: eNOS gene expression
Figure 12: TGF-β1 gene expression
Figure 13: NOS isoforms and TGF-β1 gene expression profile
We stick to your rubric like glue—nailing the structure, depth, and tone your professor wants—then polish it with edits for that extra shine. Our writers know what profs look for, and we double-check every detail to make sure it’s submission-ready and grade-worthy.
Erection dysfunction (ED), the inability to achieve and/or maintain an erection sufficient to permit satisfactory sexual intercourse (NIH, 1993), is associated with specific comorbidities such as cardiovascular disease, hypertension, diabetes mellitus (DM), lower urinary tract symptoms (LUTS), prostate cancer, depression, and obesity. ED associated with diabetes was demonstrated to be strongly related to its severity, duration, and microvascular complications (El-Sakka et al., 1999; Levy, 2002; Malavige and Levy, 2009; Glina, 2013).
ED is a prevalent global clinical problem. Approximately thirty million men are affected in the USA, with an annual increase in the diagnosis of new cases estimated by tens of thousands. Overall, the incidence of ED in the 40-70 years of age population is 52% (Feldman et al., 1994). Nevertheless, DM patients are diagnosed with ED at an earlier age, with a 78% prevalence; 6, 36 and 36% for mild, moderate and severe ED (Hakim and Goldstein, 1996; Meena et al., 2009; Seid et al., 2017).
Recent regional study stated that 86.1% of patients with type II DM had variable degrees of ED, 7.7%, 29.4% and 49.1%. for mild, moderate and severe degrees of ED. Moreover, prolonged history of DM >10 years tripled the incidence of ED compared to those who have the disease for <5 years (El-Sakka and Tayeb, 2003).
The pathophysiology of ED associated with DM is multifactorial; including neuropathy and arteriopathy, where impaired neural and endothelium-dependent mechanisms alter normal corporal smooth muscle relaxation. In addition, DM leads to abnormal endothelial function, decreased nitric oxide synthase (NOS) activity, oxidative stress-mediated neurovascular alterations, and increased cavernous tissue apoptosis (Neves, 2013). In the majority of these patients, abnormal smooth muscle responsiveness may be the underlying cause, leading to penile arterial insufficiency and venous leakage (Fuchs et al., 1989; Tamás and Kempler, 2014).
Send us your draft and tell us your goals—we’ll refine it, tightening arguments and boosting clarity while keeping your unique voice intact. Our editors work fast, delivering pro-level results that make your paper pop, whether it’s a light touch-up or a deeper rework.
Penile erection is manifested by the transformation of erectile tissue and vasculature from a state of minimally perfused flaccidity into an engorged one and mediated by a multifaceted succession of neural and vascular components, coupled with hormonal and psychologic factors. Vascular smooth muscle relaxation vasodilates arterioles and trabecular smooth muscle sinusoids which increase penile blood flow that result in compression of subtunical venules against the tunica albuginea and occlude the venous outflow (Carson and Lue, 2005; Gratzke et al., 2010).
DM produces both abnormal corporal smooth muscle cell (SMC) relaxation and generalized fibrosis of arterial media; these processes seem to uniformly underlie corporal veno-occlusive dysfunction (CVOD) (El-Sakka and Yassin, 2010).
Many classifications have been proposed for ED; the classification that integrates the various causes of ED with erectile physiology and functional anatomy is the recommended one. (Carrier et al., 1993). Clinically, an older patient with a long history of DM and vascular disease is likely to have ED secondary to vascular and neuropathic disease (El-Sakka, 2012; Glina et al., 2013).
The nitric oxide (NO)-cyclic guanosine monophosphate (cGMP) signaling pathway plays a critical role in the physiology of penile erection and in the pharmacological management of ED. Thus, NO produced by constitutive neuronal and endothelial NOS is released from nerves (nNOS) and endothelium (eNOS) upon sexual stimulation and relaxes corpus cavernosum and arterial smooth muscle to increase blood flow to the cavernous sinusoids and elicit penile erection (Burnett et al., 1992; Prieto, 2008).
The role of transforming growth factor-beta (TGF-β) is involved in numerous vital processes including inflammation, stimulation of intercellular matrix formation, production of fibroblasts, and normal healing. While growing evidence implicates TGF-β as a cytokine, vital to tissue repair, its excessive action may be responsible for tissue damage caused by scarring in many serious diseases (Ul-Hasan et al., 1998; El-Sakka et al., 1999). The pathological consequences of the action of TGF-β have been referred to as the ‘dark side’ of tissue repair (Border and Ruoslahti, 1992). DM-associated ED is associated with increased extracellular matrix deposition that could be due to increase of cytokines such as TGF-β and reduced smooth muscle content in the corpus cavernosum. The mechanisms of these processes are not well-understood (El-Sakka et al., 1999; Zhou et al., 2012).
Yes—we’ve got your back! We’ll brainstorm fresh, workable ideas tailored to your assignment, picking ones that spark interest and fit the scope. You choose the winner, and we’ll turn it into a standout paper that’s all yours.
Phosphodiesterases (PDEs) are distributed throughout various tissues; primarily in the vascular, visceral and pulmonary smooth muscles. In the penis, PDE-5 causes breakdown of cGMP, where its inhibition increases its bioavailability facilitating NO-mediated relaxation of erectile smooth muscle with sexual stimulation. (Beavo, 1995).
Conventional Phosphodiesterase 5 inhibitors (PDE5Is) include sildenafil, vardenafil, tadalafil and avanafil. New PDE5Is include udenafil and mirodenafil. PDE5Is exhibit analogous modes of action. However, they vary in their pharmacodynamics and pharmacokinetics. Sildenafil was Food and Drug Administration (FDA)-approved in 1998, vardenafil and tadalafil in 2003 and avanafil in 2012. Vardenafil is the most potent of the three in inhibiting PDE5 activity while tadalafil was reported to have extended plasma half-life up to 18 h as compared to 3–4 h in the case of sildenafil and vardenafil (Wright, 2006; Ismail and El-Sakka, 2016, 2017).
Vardenafil was effective in treating DM-induced ED with the greatest effect achieved through chronic dosing; with no additive effect measured with the final acute dose (De Young et al., 2008). Changes noted in the histology and protein expression indicate that vardenafil may have a protective effect in this disease state. Furthermore, vardenafil is a candidate therapy for the rehabilitation of patients with DM (Ferrini et al., 2006). Furthermore, recent study investigated the functional and structural changes of penile cavernous tissue after administration of low-dose tadalafil. They concluded that low-dose chronic administration of tadalafil is associated with structural and functional improvement of erection (Mostafa et al., 2013).
Rationale: due to the inability to collect human samples to investigate the effect of early versus late administration of vardenafil in DM patients with ED, this fact prompted us to investigate this effect in a rat model.
To determine the possible prevention of deleterious consequences of DM on erectile function with administration of PDE5 inhibitors.
Yep—need changes fast? We’ll jump on your paper and polish it up in hours, fixing whatever needs tweaking so it’s ready to submit with zero stress. Just let us know what’s off, and we’ll make it right, pronto.
Study Objectives
Primary objective
To investigate the effect of early versus late administration of vardenafil on erectile function in a rat model of diabetes.
Secondary objective
To identify Intracavernosal pressure (ICP), histopathological and ultrastructural changes, plus eNOS, nNOS, inducible (iNOS) and TGF-β1 genes expression in a rat model of diabetes after early versus late administration of vardenafil.
Study question
Sure thing! We’ll whip up a clear outline to map out your paper’s flow—key points, structure, all of it—so you can sign off before we dive in. It’s a handy way to keep everything aligned with your vision from the start.
Does early administration of vardenafil prevent ED in a rat model of diabetes?
Study hypothesis
Early administration of vardenafil will prevent ED in a rat model of diabetes.
ED is a prevalent worldwide clinical condition that will be escalated up to 322 million by 2025, compared to 152 million in 1995 (McKinlay, 2000; El-Sakka, 2017). ED is prevalent in the middle-east community and reach up to 92.6% in those individuals. In addition, about 50.8% of patients with sexual disorders presented with premature ejaculation and 7.6% presented with low sexual desire. Moreover, 80% had organic and 20% had psychogenic causes of ED. Mild, moderate and severe ED was diagnosed in 10%, 40% and 5% respectively (Brock, 2000; El-Sakka, 2004).
The prevalence rate of ED was reported 63.6%, in Egypt, 57.4% in Nigeria and 80.8% in Pakistan (Seyam et al., 2003; Shaeer et al., 2003). Consequently, There have been a phenomenal improvement in the diagnosis and treatment of ED in the last three decades (Ismail and El-Sakka, 2016, 2017; El-Sakka, 2017).
The cornerstone of erectile function is an incorporated process of vascular and neural functions that promote trabecular smooth muscle relaxation, leading to distention of sinusoidal spaces and blood inflow into corpora cavernosa, facilitating penile erection. This process employs mechanical compression of emissary veins integrated in the tunica albuginea causing impedance of blood flow that eventually results in penile erection (El-Sakka and Lue, 2004). Autonomic nervous system delivers sympathetic (T12–L2) and parasympathetic (S2–S4) innervation to pelvic plexus, counting the cavernous nerves. Autonomic nerve fibers are responsible for NO delivery that results in trabecular smooth muscle (SM) relaxation (Andersson and Wagner, 1995; Burnett, 1997).
Absolutely—we’ll weave in sharp analysis or eye-catching visuals like stats and charts to level up your paper. Whether it’s crunching numbers or designing a graph, our writers make it professional and impactful, tailored to your topic.
Acetylcholine (ACH) is essential for ganglionic transmission (via nicotinic receptors) and vascular SM relaxation (via muscarinic receptors). Cholinergic nerves were identified within cavernous SM and neighboring penile arteries. ACH stimulates NO release from endothelial cells and potentiates direct SM relaxation during erection (Sáenz de Tejada et al., 1988)
Vasoactive intestinal polypeptide VIP is one of the neurotransmitters involved in penile erection. Immune-reactive VIP nerve fibers were identified inside the cavernous trabeculae and surrounding cavernosal arteries. Cavernosal SM relaxation is blocked by VIP antagonists (Kim et al., 1995). Other neurotransmitters include calcitonin-gene-related peptide (CGRP) (Stief et al., 1990), histidine methionine peptide (Kirkeby et al., 1992), pituitary adenylate cyclase activating polypeptide (Hedlund et al., 1994) 32 and prostaglandins (PGs) (Saenz de Tejada et al., 1989). Density of prostaglandin E1 receptor is decreased in men with ED (Aboseif et al., 1993). Vascular tone’s neural-endothelial control and neuromodulators/neurotransmitters interactions at neuromuscular junction have been also investigated (Andersson and Holmquist, 1994).
NO stimulates guanylate cyclase production of cGMP; this reduces cytosolic calcium concentration and eventually facilitates trabecular SM relaxation and increase blood flow into sinusoidal spaces (Sáenz de Tejada, 2002). This pathway is reversed by PDE5 enzymes by cGMP inactivating, resulting in cytosolic calcium concentration and smooth-muscle contraction. Sacral spinal cord provides motor nerve supply through pudendal nerve innervation. Pudendal nerve fibers join the ischio-cavernosus and bulbo-cavernosus muscles (Stief et al., 1998).
Sympathetic stimulation results in detumescence via cavernous smooth-muscle contraction, while cholinergic stimulation may facilitate erection through sympathetic inhibition in addition to endothelial NO release (Sáenz de Tejada et al., 1988). Corporeal SM relaxation is essential for normal erectile function, and evidence implicated that nNOS and eNOS are the principal mediators of SM muscle relaxation (Hurt et al., 2002). NO is synthesized from the precursor, L-arginine substrate via the catalytic activity NOS enzyme (Rajfer et al., 1992).
Penile erection is essentially a neurovascular mechanism that primarily requires initiation followed by maintenance of tumescence through corporeal SM relaxation and increased blood flow to the penis. The production and release of NO (by endothelial cells and nitrergic nerves) are widely accepted to be the pacemaker of physiological erection; depending on NO-cGMP signaling transduction pathway. If any factor involved in this cascade is affected, ED ultimately will occurs (Burnett and Musicki, 2005).
cGMP upregulation facilitates SM relaxation, through cGMP-dependent protein kinase activation. Consequently, Potassium (K+) channel activity increase and intracellular calcium (Ca2+) concentrations decreases (Bivalacqua et al., 2003).
Lack of the number of NOS-containing nerve fibers, NOS activity and endothelial SM relaxation impairment are the major contributing factor to ED in DM patients. Some studies established that eNOS and nNOS downregulation of their protein and gene expression in DM animal models are the main factors of erectile function impairment (Bivalacqua et al., 2001)
Meanwhile, these researches recognized a possible mechanism for ED development in DM patients; that is a decrease in production of NO, through reduction in nNOS and eNOS in corporeal vasculature (Akingba and Burnett, 2001).
Genetic studies have successfully implicated methods of increasing the transduction of a desired gene through gene transfer technologies. Gene transfer enhances gene expression and the functional activity of the desired gene. nNOS and eNOS gene transfer into penile tissue, vehicle on adenovirus has effectively reversed age-related ED in a rat model (Thomas R Magee et al., 2002).
Previous studies showed that NOS isoforms gene transfer can enhance physiological profile of penile tumescence in vivo; thereby, NOS expression improved ED associated with NOS downregulation. The effects of eNOS gene transfer into the penis of STZ-induced DM rats was being investigated; and it was concluded that erectile function could be improved if NO expression is restored (T R Magee et al., 2002). eNOS is an essential element of erectile function; it has the capability of inducing vasodilation and inhibition of vasoconstriction (Montorsi et al., 2004).
We tackle each chunk with precision, keeping quality consistent and deadlines on track from start to finish. Whether it’s a dissertation or a multi-part essay, we stay in sync with you, delivering top-notch work every step of the way.
On the other hand, testosterone (T) directly affects endothelial function. NO is the pacemaker of endothelial function; its bioavailability is markedly decreased with T deprivation. Therefore, T may possess direct influence on endothelial function and migrating endothelial progenitor cells (EPC) (El-Sakka, 2017).
TGF-β1 molecule is isolated from platelets, human placenta and bovine kidney. It has a (25kD) homodimer molecular composition (Sporn and Roberts, 1992).
TGF-β1 action in tissue repair process, involves a complexed sequences of cytokine production, monocyte chemoattraction, angiogenesis and additional inflammatory mediators (Border and Ruoslahti, 1992). Moreover, TGF-β1 triggers matrix components synthesis; including tenascin, proteoglycans, collagens and fibroactin (Balza et al., 1988). In the same time, it concomitantly blocks matrix degradation by blocking protease synthesis and stimulating proteases inhibitors leading to accumulation of extracellular matrix (ECM) deposition at tissue injury site, This results into fibrosis and scarring. Moreover, TGF-β has the ability to self-control its own production; this may be the key to persistence of fibrosis and scarring (Border and Ruoslahti, 1992).
Previous studies had demonstrated the role of TGF-β in a rat model of Peyronie’s disease. they found that TGF-β2 and TGF-β3 had no remarkable protein expression, while TGF-β1 gene expression in the cytomodulin-injected rats was noted after 2 weeks post-induction (El-Sakka et al., 1997a, 1997b; El-Sakka et al., 1998).
From a similar perspective, other authors investigated the role of TGF-β1 in a canine model of prolonged penile erection; they related an association between prolonged penile erection with a relatively increased TGF-β gene expression as a moderator of fibrosis; with a resultant structural and morphological changes in a short period of time, suggesting that early therapeutic intervention with agents that counteract TFG-β action may be a desirable treatment modality (El-Sakka et al., 1998).
Yes—we’ve got it down! Our writers switch seamlessly between UK, US, Australian, or any other standards, matching your school’s exact expectations. Your paper will feel native to your system, polished and ready for wherever you’re studying.
Collectively, TGF-β1 Gene and its expression have been found to be elevated in animal models with fibrotic conditions in various tissues (e.g. lung and liver) (Balza et al., 1988; Castilla et al., 1991; El-Sakka et al., 1997); Nevertheless, some previous studies couldn’t elicit any difference in TGF-β1 gene expression in an animal model of diabetes compared to control. However, other growth factors may play a role in that perspective (El-Sakka et al., 1999).
There was a previous thinking referred ED to psychogenic causes only, especially in younger population. However, with the advances of ED research, it is strongly believed now that there are other organic causes contribute to ED such as hormonal, neural, pharmacological and penile factors specifically in older patients (Fazio and Brock, 2004).
Some neurologic disorders are associated with ED, including multiple sclerosis (MS), stroke, epilepsy, Alzheimer’s disease, Parkinson’s disease, spinal cord injury and radical pelvic surgeries (e.g., radical prostatectomy) (Siddiqui et al., 2012).
Liver disease, prostate disease, LUTS, pelvic surgery and renal failure lead to exposure physical inactivity. Use of recreational drugs, caffeine consumption, drug addiction and pelvic surgery are also reported as risk factors associated with the pathophysiology of ED (El-Sakka, 2012a).
DM is a chronic disease characterized by absolute or relative deficiency of insulin, which consequentially lead to hyperglycemia. Prolonged hyperglycemia may lead to serious complications such as nephropathy, neuropathy and retinopathy and increased cardiovascular risk (Hyttinen et al., 2003).
Progressive delivery is a cool option where we send your paper in chunks—perfect for big projects like theses or dissertations. You can even pay for it in installments. It’s just 10% extra on your order price, but the perks are worth it. You’ll stay in closer touch with your writer and can give feedback on each part before they move to the next. That way, you’re in the driver’s seat, making sure everything lines up with what you need. It saves time too—your writer can tweak things based on your notes without having to redo huge sections later.
A total of 4556 patients; 1494 from Egypt, 2162 from Saudi Arabia and 900 from the United Arab Emirates were observed for ED treatment with PDE5I. DM was the most frequent diagnosis in 76% of these patients, primarily type II DM (67.5 of all patients). Symptoms of peripheral neuropathy were the most commonly reported complications of DM. Hypertension was reported in 36.3% of patients, dyslipidemia in 66.7% and coronary heart disease in 15.7% of patients (El-Sakka et al., 2011)
Type II diabetes is associated with diminished beta cell compensation of insulin resistance that eventually lead to insulin deficiency. Lifestyle modification, exercise and weight reduction may improve Insulin resistance (Solomon et al., 2008). DM, dyslipidemia, arterial hypertension, depression and coronary artery disease (CAD) are the main risk factors for the development of ED (Glina, Sharlip and Hellstrom, 2013).
Latest estimates from the International Diabetes Federation (IDF) is that in 2015 there were 415 million people with DM worldwide. By 2040, this number is anticipated to rise to 642 million. World Health Organization (WHO) and non-communicable diseases (NCDs) risk factor collaboration provided a similar estimation of 422 million cases in 2014 (Zimmet et al., 2016)
Prevalence of both diagnosed and undiagnosed DM in Egyptian population aged more than 20 years is estimated to be 9.3% (Herman et al., 1995). Recent studies estimated the prevalence of type II DM in the Egyptian population approximately 15.6% of all adults (20-79) years of age (Hegazi et al., 2015). Several studies in the Middle East disclosed a more than 40% prevalence of ED. At least 5 Arab countries were counted in the worldwide top 10 countries with a high prevalence of DM (El-Sakka, 2012a).
Absolutely! If your teacher’s got feedback, you can request a free revision within 7 days of approving your paper—just hit the revision request button on your personal order page. Want a different writer to take a crack at it? You can ask for that too, though we might need an extra 12 hours to line someone up. After that 7-day window, free revisions wrap up, but you can still go for a paid minor or major revision (details are on your order page). What if I’m not satisfied with my order? If your paper needs some tweaks, you’ve got that free 7-day revision window after approval—just use the “Revision” button on your page. Once those 7 days are up, paid revision options kick in, and the cost depends on how much needs fixing. Chat with our support team to figure out the best way forward. If you feel the writer missed the mark on your instructions and the quality’s off, let us know—we’ll dig in and sort it out. If revisions don’t cut it, you can ask for a refund. Our dispute team will look into it and figure out what we can offer. Check out our money-back guarantee page for the full scoop.
ED is an independent risk factor for reduced quality of life in diabetic patients. The association between DM and ED was addressed as high as 75% in some populations with an increased incidence of ED in diabetic patients by 68 cases/1000 patients per year (Malavige et al., 2014).
El-Sakka and Tayeb stated that 86.1% of Type II diabetic patients had some degrees of ED; including 7.7%, 29.4% and 49.1%. for mild, moderate and severe ED respectively. Twenty five percent of DM patients below 50 years of age had ED, escalated to 75% in those >50 years of age. Seventy percent of whom without ED were <50 years of age compared to 30% who were >50 years (El-Sakka and Tayeb, 2003).
Prolonged history of DM >10 years was associated with a triple increase in the risk of ED development, this is less likely in those with a <5 years history of DM. Poor metabolic control is associated with a 12.2 time increase in the risk of ED compared to a less likely occurrence in men with good metabolic control. Fifty-three percent of diabetic men with ED have ≥1 diabetes-related complications compared to 20.5% in those without ED (El-Sakka and Tayeb, 2003).
Penile doppler ultrasound changes were addressed in diabetic patients in the form of decreased peak systolic velocity (PSV) and poor response to intracorporeal injection (ICI) of vasoactive materials (El-Sakka, 2003).
Additional study evaluated the association between type II DM and Peyronie’s disease (PD) found an 8.1% prevalence of PD among a total of 1133 diabetic patients. Moreover, psychological disorders and dyslipidemia were associated with PD (El-Sakka and Tayeb, 2005). Another study concluded that type II DM and PD negatively affected the vascular status of erection, either solely and together (El-Sakka and Tayeb, 2009).
Pathogenesis of ED in diabetic patients is a multifactorial process associated with multiple endocrine, neuronal, hormonal, metabolic and vascular factors. Oxidative stress is also associated with endothelial and neuronal apoptosis leading to endothelial denudation and neuronal damage leading eventually to further depletion of NO (Russell et al., 2002). Moreover, superoxide employs calcium ion mobilization leading to direct vasoconstriction, possibly produce ED (Wan et al., 2010).
Dyslipidemia, obesity, metabolic syndrome, insulin resistance, hyperglycemia and other metabolic abnormalities are risk factors for development of ED with DM (Hidalgo-Tamola and Chitaley, 2009).
El-Sakka and colleagues investigated structural and ultrastructural changes using rat model of DM. Their study addressed functional abnormalities using cavernous nerve electrostimulation. Electrostimulation was lower in diabetic rats compared to control group. DM rats had short-lived stimulation curve, as it initiated after a latency period with a short curve duration and premature decline in pressure curve before the end of stimulation. They also found significant down-regulation of NOS isoforms (nNOS and iNOS) in diabetic rats with normal expression of TGF-β1 in both diabetic and control rats and no eNOS expression was elicited in all groups (El-Sakka et al., 1999).
Diabetes-related ED was found to be associated with variable degrees of corporeal fibrosis and vascular smooth muscle (VSM) apoptosis (Kovanecz et al., 2009). Corporeal tissue, like any other tissue is exposed to overproduction of plasminogen-activator inhibitor 1, upregulation of reactive oxygen species (ROS) and TGF-β1 activation (Gonzalez-Cadavid and Rajfer, 2010). Vascular elasticity is jeopardized when fibrosis of arterial tunica media increases, eventually leading to plaque formation, an effect which could be postponed or reversed via PDE5Is administration (Kovanecz et al., 2009).
PDE5Is are the standard drugs for ED treatment since sildenafil citrate was FDA-approved in 1998, consequently; other agents such as vardenafil, tadalafil, and avanafil have gained popularity as an effective ED oral treatment (Ismail and El-Sakka, 2017). PDE5Is have been rapidly considered as the patient-friendly ED treatment method and currently they are recommended as the first-line monotherapy (Lue T, 2006).
PDE5Is act by facilitation of cavernous SM relaxation via inhibition of cGMP, the catalytic enzyme involving NO degradation. PDE5Is are solely effective under the influence of sexual stimulation. Their effect is to potentiate rather than to initiate penile erection via NO release in the first place (Burnett, 2005). Overall, the satisfaction rate of PDE5 inhibitors administration is approximately 70% (Khera and Goldstein, 2011).
Vardenafil (Levitra, Bayer) is a super-selective and strong PDE5 inhibitor. Regardless of being similar in its chemical structure to sildenafil, it is more effective and selective than it. It’s recommended starting dose is 10 or 20 mg orally (Levitra®) or 10 mg sublingually (Staxyn®). Vardenafil exhibits a rapid onset of action, compared to other PDE5Is. AT 25 min, nearly 53% of patients can get erection sufficient for penetration. Vardenafil absorption, like other PDE5Is, is diminished after a fat meal (Rajagopalan et al., 2003). Dose-dependent adverse effects include dyspepsia (6%), headache (21%) and flushing (13%) (Montorsi et al., 2004).
PDE5Is increase NO synthesis and reduce insulin-resistance in endothelial cells. Tadalafil treatment in type II diabetic patients aggravates capillary employment and enhances skeletal muscle glycaemia (Jansso et al., 2010).
From a different perspective, PDE5Is were found to reduce glomerular hypertrophy and downregulates matrix metalloproteinase-2 (MMP-2), type I and II collagen and matrix metalloproteinases tissue inhibitor in the kidney of DM animal model (Kuno et al., 2011). PDE5Is also exhibited some blunting of mesangial cell fibrosis and proliferation and downregulates TGF-β signaling and activation proteins; p-smad-2/3 and TSP-1 (Hohenstein et al., 2008).
PDE5Is also diminish fibrotic changes in a cardiac hypertrophy animal model (Nagayama et al., 2009). Furthermore, in a model of insulin-resistance and diet-induced obesity, low-dose chronic administration of PDE5Is reduces collagen deposition and insulin resistance in skeletal muscles (Kang et al., 2011).
At the first to 8th week, progressive protein buildup occurs in the corpus cavernosum and vascular smooth muscle in a rat model of diabetes after STZ administration and induction of chemical hyperglycemia (Yohannes et al., 2010). These outlines may give some clues to the ameliorating effect of PDE5Is and their anti-fibrotic actions in diabetes-induced ED and further diseases.(Francis and Corbin, 2011)
Early administration of conventional PDE5Is is thought to be the first-line method to ameliorate the deleterious effect of DM in these patients (L. et al., 2012). Nevertheless, nearly half of these patients may not respond very well. The protective effect of PDE5Is in diabetic patients is achieved via interaction of PDE5Is with the its catalytic site, hence cGMP breakdown is blocked, leading to upregulation of cGMP in the corpora cavernosa (Choi et al., 2015).
Endothelial dysfunction is the principal mechanism that lead to development of ED with DM, the use of PDE5Is improves basically this mechanism. This is likely to be a result of increased cavernosal blood flow in addition to changes in cellular functions, gene transcription, metabolic processes and calcium homeostasis. There’s a progressive decline in the VSM and endothelium of diabetic men’s cavernosa. Moreover, an amplification of endothelial dysfunction and pro-inflammatory processes ensues in diabetic patients with ED (Usta et al., 2006; Araña Rosaínz et al., 2011).
Increased circulating levels of endothelial dysfunction marker (E-selectin), and elevated inflammatory marker; Tumor necrosis factor-alpha (TNF-α) and low interleukin (IL-10) is encountered in diabetic patients with ED. There’s also positive correlation between cavernosal levels of advanced glycation end products (AGEs) and diabetes-related ED (Araña Rosaínz et al., 2011).
In hyperglycemic conditions, there’s a buildup of AGEs which by its role intermingle with receptor for AGE receptor (RAGE) leading to upregulation of monocyte chemo-attractant protein-1 (MCP-1), that is responsible for tissue damage that occurs with diabetes (Ramasamy, Yan and Schmidt, 2011; Neves, 2013).
In endothelial cells, vardenafil decreases AGE- mediated surge in RAGE and generation of ROS, so downregulates MCP-1 mRNA (Ishibashi, Matsui, Takeuchi and S. I. Yamagishi, 2011). This effect is mediated by NO/cGMP pathway. Moreover, in diabetic models, ED is reversed by inhibition of AGE formation (Usta et al., 2006).
eNOS is found to decrease in a rat model of obesity, where insulin resistance and inflammation occurs. This effect is ameliorated by PDE5Is administration, however, animals on low-fat diet seems to lack this effect (Rizzo et al., 2010).
Endothelial function is improved following continuous administration of low-dose PDE5I; an effect which is lasted for a significant period after cessation of treatment (Burnett et al., 2009). This effect is augmented by the addition of antioxidant therapy to PDE5I regimen; consequently, a maintained efficacy is encountered for at least 4 weeks post-treatment (Morano et al., 2007). This process is associated with downregulation of P-selectin, intercellular adhesion molecule-1 and other inflammatory markers. Daily administration of low-dose PDE5I for a month reduces enothelin-1 level in type II diabetic rats (Ritchie and Sullivan, 2011).
PDE5Is treatment in type II diabetic patients upregulates flow-mediated dilatation and downregulates endothelin-1 levels; enhances nitrite/nitrate levels and decreases vascular inflammatory markers (Aversa et al., 2008).
Previous studies demonstrated that insulin resistance reduces eNOS and AKT-1 activation which are restored via PDE5Is administration (Mammi et al., 2011). In an animal model of diabetes, PDE5Is were found to down-regulate oxidative stress, and inhibits p47phox (a NADPH oxidase active subunit, that mainly provides superoxide ions that abolish NO bioactivity and decreases PDE5 expression (Shukla et al., 2009).
The once daily regimen of PDE5Is was reported as a valuable substitute to on-demand PDE5I treatment in ED patients (Hatzichristou et al., 2015; Kim et al., 2015). It was found that >68% of patients on once-daily regimen of PDE5Is could withstand this treatment plan for 6 months (Buvat et al., 2014).
In another perspective of PDE5Is use in treatment of DM-associated ED, amelioration of DM effect on potency was attained by chronic low-dose PDE5I administration mutually by strict control of blood sugar levels (Choi et al., 2015). Likewise, insulin sensitivity and endothelial function were boosted on a 3-months PDE5I regimen (Buvat et al., 2014). PDE5Is increase intracellular cGMP via enhancing NOS in a rat model of diabetes-induced ED in the cavernosal tissue via improvement of nNOS gene expression and increase NOS activity (Zhang et al., 2012).
This study is a prospective experimental investigation. The study was carried-out at the animal house and research Lab., Faculty of Medicine, Suez Canal University, Egypt. This experimental work was carried out on a total of 60 adult male Albino Wistar rats; aged 60-80 days and weighed 150-200 grams each. Animals were brought from the national research center for experimental animals, Cairo.
Environmental conditions were standardized for all animals. All rats were kept for at least one week prior to the experiment to be adapted. Each animal was assigned a unique identification number (foot tag). Animals were assigned to sham, DM without treatment and treated groups in a simple random manner; this helped to minimize bias and assure comparability of pertinent variables across groups. Rats were divided into six groups of 10 rats each:
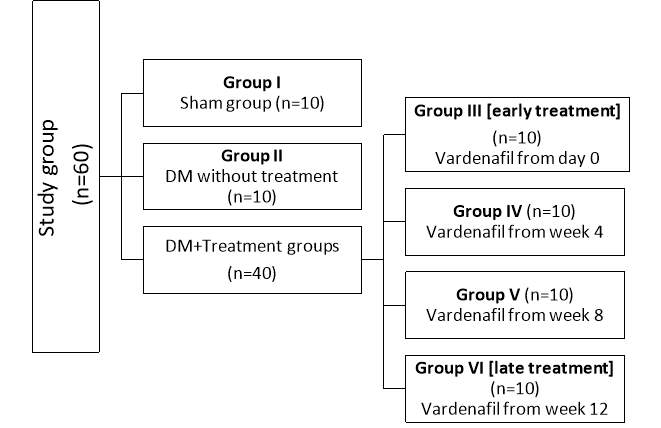
DM was induced by two low-dose with two weeks interval of intraperitoneal injection of 25 mg/kg Streptozotocin (STZ; 2-deoxy-2-(3-(methyl-3-nitrosoureido)-D-glucopyranose; Sigma, St. Louis, MO) in a citrate buffer (pH 7.0, 100 mMol citric acid, 200 mMol di-sodium phosphate).
Three days after the second dose of STZ, blood samples from the tip of rat’s tail were obtained under aseptic conditions, for determination of blood glucose level. Candidate DM rats with blood glucose levels above 300 mg/dL were assigned as the sample of the study (Lukić et al., 1998).
Groups III, IV, V and VI were subjected to chronic vardenafil treatment (Levitra, Bayer Healthcare Pharmaceuticals Inc., Wayne, NJ 07470, Germany). Chronic vardenafil treatment was given by daily oral gavage according to the schedule in a dose of 0.5 mg/kg (equivalent to 0.1 mg/200 g) weight daily (De Young et al., 2008).
The sham group was euthanized at 12 weeks of start of the experiment. DM group without treatment was euthanized at 12 weeks after induction of DM. Each treatment group received chronic vardenafil treatment for 12 weeks before euthanization and tissue harvesting. Functional study assessment of all groups was performed before euthanization and tissue harvesting.
Intracavernosal pressure in response to cavernous nerve stimulation was measured and recorded using BIOPAC MP150® data acquisition system (TSD104A blood pressure transducer, STMISO nerve stimulation adapter, BIOPAC Systems Inc., 42 Aero Camino, Goleta, CA 93117, USA, 2011) connected to computer device using AcqKnowledge® software for data analysis version 4.1 (BIOPAC Systems Inc., 42 Aero Camino, Goleta, CA 93117, USA, 2009). Mean arterial blood pressure (MAP) was measured and recorded by means of tail-cuff measurement, following instructions supplied by the manufacturer (NIBP200A non-invasive Blood Pressure System, BIOPAC Systems Inc., 42 Aero Camino, Goleta, CA 93117, USA, 2011).
Rats of each group were surgically explored for direct electrostimulation of the cavernous nerve. Under general anesthesia using intra-peritoneal pentobarbital sodium (35 mg/kg), each rat was placed on a heating pad to maintain its body temperature at 37ο C. Through a lower abdominal midline incision, the area postero-lateral to the prostate was explored on both sides. Major pelvic ganglia, pelvic nerves and cavernous nerves were identified and exposed. The skin overlying the penis was incised and both penile crurae were exposed by removing part of the overlying ischio-cavernous muscle (El-Sakka et al., 1999).
A 23 Gauge butterfly cannula filled with 250 Unit/ml of heparin solution was connected to PE-50 tube and was inserted in the right crus for ICP measurement. Cavernous nerve electrostimulation was performed using a delicate stainless-steel bipolar hook electrode (each pole is 0.2 mm in diameter; the two poles were separated by 1 mm). Computer generated monophasic rectangular pulses with a custom-built constant current amplifier. Stimulus parameters were; current 1.5 mA, frequency 20 Hz, pulse width 0.2 ms, and duration 50 s.
After functional study is completed, a 2-mm penile segment was taken for histopathological examination of the cavernous tissue. The collected tissue was immediately placed in 10% formalin solution. Another 2-mm of cavernosal tissue was taken; fixed in 2.5% glutaraldehyde in 100 mM phosphate buffer at pH 7.0 at 4°C for 24 hours for transmission electron microscopy (TEM).
A different penile segment was taken and kept in -70ο C freezer until it was processed for real-time polymerase chain reaction (RT-PCR) and assessment of messenger ribonucleic acid (mRNA) expressions of eNOS, iNOS, nNOS and TGF-β1 genes. Blood sample from each rat was obtained by direct suction from the heart and sent for serum glucose estimation.
The 2-mm penile segments were preserved in 10% formalin solution and dehydrated in ascending grades of alcohol. After xylene treatment, the specimens were embedded in paraffin blocks. 5 µm thick sections were cut by microtome and stained with hematoxylin and eosin (H&E) and Masson trichrome staining. The stained sections were examined using light microscope (Bancroft et al., 2008).
H&E sections were examined for determination of trabecular smooth muscle architecture, mass and cavernosal spaces. Masson trichrome were examined for determination collagen matrix deposition, smooth muscle content, areas of fibrosis and smooth muscle to collagen ratio.
All histopathology images were captured using:
Quantitative image analysis
Two millimeters from the cavernosal tissue was selected for ultrastructural examination by TEM for demonstration of ultrastructural changes (e.g.; area of smooth muscles, elastic tissue, fibrous tissue, microfibrils, structure of the myelinated nerve fibers, endothelium, nuclear chromaticity, mitochondrial and cytoplasmic changes), post-fixed for 1 h in 1% osmium tetroxide dissolved in phosphate buffer, dehydrated in 30% ethyl alcohols and embedded in epoxy resin at 40-60o C.
Transmission electron microscope was used to examine the samples (JEOL Electron Microscope; JEM-2100, JEOL Ltd., 3-1-2 Musashino, Akishima, Tokyo 196-8558, JAPAN).
Quantitative analysis of TGF-β1 and NOS isoforms (eNOS, nNOS, iNOS) gene expression was done in the following steps:
Samples were obtained from cavernous tissue of the rat to quantitatively measure the eNOS, nNOS, iNOS and TGF-β1 genes using quantitative Real-Time PCR (qRT-PCR) technology.
by following the protocol supplied by the manufacturer (QIAGEN, RNeasy Mini Kit, Catalog no. 74104); by tissue disruption using a mortar and pestle. Freezing the animal tissue immediately in liquid nitrogen and grind to a fine powder under liquid nitrogen. Transfer the suspension (tissue powder and liquid nitrogen) into appropriately sized tube and allows the liquid nitrogen to evaporate without allowing the sample to thaw.
The ratio of the readings at 260 nm and 280 nm (A260/A280) was examined to provide an estimate of the purity of RNA with respect to contaminants that absorb in the ultraviolet (UV) spectrum. RNA with an absorbance ratio of 1.8 and 2.2 was very pure. Despite many of the RNA samples falling out of the range that would be considered a “pure” RNA sample, they all maintain the ability to amplify our target gene through RT-PCR.
It is a two-step approach; reverse transcription (RT) to convert RNA to complementary deoxyribonucleic acid (cDNA) using RT primer and reverse transcriptase, followed by PCR analysis using TaqMan® assay (Applied Biosystems, assay ID 000397, catalogue no 4427975, Egypt); Taqman® Universal PCR master mix II, No Uracil-N glycosylase (UNG) (Applied Biosystems™, Catalogue number 4440038); Taqman® gene expression TM assay (20×); (Custom TaqMan® Gene Expression Assay Catalogue number 4331348) (Schmittgen and Livak, 2008).
TaqMan® Endogenous control assay, labeled with FAMTM as a reporter dye was used to normalize the expression levels of eNOS, iNOS, nNOS and TGF-β1 to correct any possible differences in RNA quantity or quality across samples.
RT-PCR allows accumulating amplified cDNA to be detected and measured as the reaction progresses. The reaction consists of an exponential phase, in which the amount of amplified product, detected by incorporated fluorescently-labeled gene-specific probe in the reaction, approximately doubles during each cycle of denaturation, primer annealing and template extension, and a non-exponential or plateau phase in which reduced reagents limit the reaction. The point at which enough amplified product has accumulated to produce a detectable fluorescent signal is known as the threshold cycle or (CT) and the greater the amount of starting template, the lower the CT value. The threshold of different runs across samples for same experiments was adjusted to be the same for comparison.
Quantification of gene expression was estimated using relative quantification method to quantify differences in the expression level of gene between different samples. The expression levels of genes were normalized by the expression level of Glyceraldehyde 3-phosphate dehydrogenase (GAPDH). The mean and standard deviation values of the replicate sample results were calculated in Microsoft® Excel software. The fold changes in gene expression (ΔΔCT) were calculated by 2(-ΔΔCT) (Schmittgen and Livak, 2008).
Assessment of gene expression by gel electrophoresis:
The integrity of the extracted cDNA was assessed by performing DNA gel electrophoresis at 2% concentration of agarose (Cat #PMI080-011EVI, Biosciences (Axygen), Spain) in 1X Tris borate EDTA running buffer (TBE) (Cat #B5, Fermentas, Lithuania). Ethidium Bromide 10mg/ml (Cat # H5041, Promega Corporation, Madison, USA); Blue/Orange 6x Loading Dye (Cat# G1881, Promega Corporation, Madison, USA). With utilization of horizontal slab gel electrophoresis apparatus, Microwave oven and UV-Illuminator (San Gabriel, CA, USA).
DNA sample was loaded into a well of agarose gel and then exposed to an electric field. The negatively charged DNA backbone migrates to the anode. Since small DNA fragments migrate faster, the DNA is separated by size. The percentage of agarose in the gel determined what size range of DNA resolved with the greatest clarity. NOS isoforms (eNOS, iNOS and nNOS) and TGF-β1 Genes expression of sham, DM control and treatment groups; and the different base pairs length of different expressed genes were assessed.
Sample size justification:
Sample size calculation using the equation of the difference between two means (Dawson and Trapp, 2004):
Sample size / group: n = 2σ2 (Zα + Zβ)2 / Δ2
Where:
| Zα |
You Want The Best Grades and That’s What We Deliver
Our top essay writers are handpicked for their degree qualification, talent and freelance know-how. Each one brings deep expertise in their chosen subjects and a solid track record in academic writing.
We offer the lowest possible pricing for each research paper while still providing the best writers;no compromise on quality. Our costs are fair and reasonable to college students compared to other custom writing services.
You’ll never get a paper from us with plagiarism or that robotic AI feel. We carefully research, write, cite and check every final draft before sending it your way.